Melanotan II 5mg
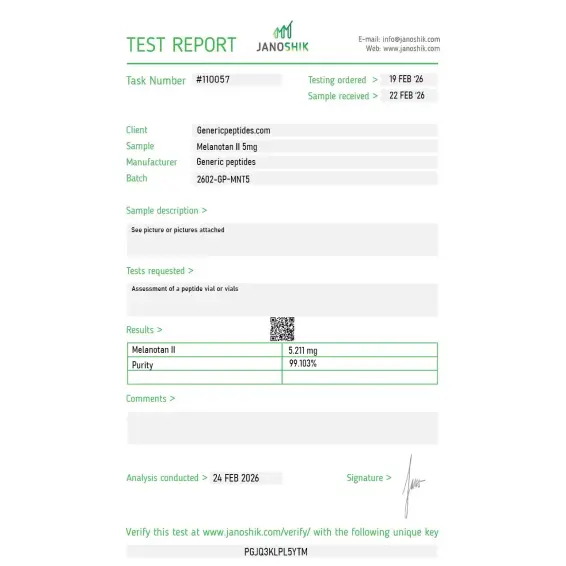
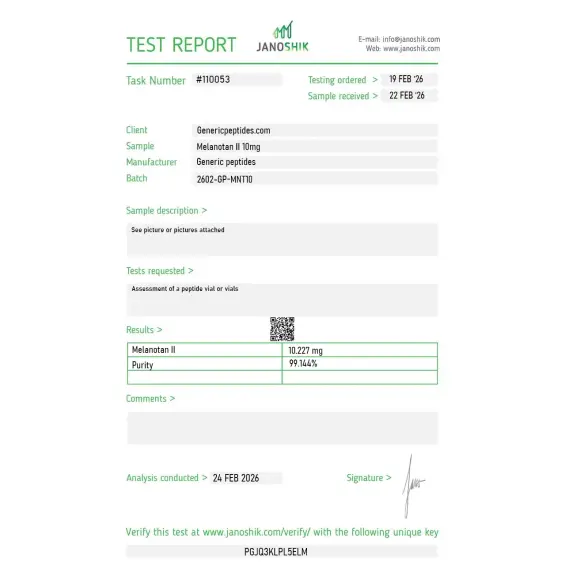
Certificate of Analysis available




The University of Arizona research team developing Melanotan II in the 1980s wasn't trying to invent a tanning drug. They were trying to prevent skin cancer — engineering a stable analog of α-MSH that would induce melanin production without requiring UV exposure. Decades later, the compound failed pharmaceutical development, got banned in multiple countries, and somehow became the most-discussed peptide in beauty forums anyway. The story of how that happened is the entire reason this page exists.
Melanotan II (MT-II) is a synthetic cyclic heptapeptide — a 7-amino-acid analog of α-melanocyte-stimulating hormone (α-MSH). The natural α-MSH peptide regulates skin pigmentation by binding melanocortin receptors, but it's biologically unstable and impractical as a research or therapeutic tool. The Arizona team modified the sequence to create a much more stable, more potent analog with broad melanocortin receptor activity.
That's the structural part. What makes MT-II pharmacologically distinct from its sibling Melanotan I (afamelanotide, FDA-approved as Scenesse for erythropoietic protoporphyria): MT-II is a non-selective melanocortin receptor agonist. It hits multiple melanocortin receptor subtypes — MC1R (pigmentation), MC3R and MC4R (appetite, sexual function, energy balance) — simultaneously. The non-selectivity is what gave Melanotan II its strange research profile: pigmentation, appetite suppression, and effects on sexual function all came from the same compound.
MT-II's pharmaceutical development stalled in clinical trials. The non-selectivity that made it interesting also made it problematic — controlling pigmentation while avoiding nausea, blood pressure changes, and unwanted sexual effects proved too difficult for a commercial drug. Afamelanotide (Melanotan I) was advanced instead, with cleaner MC1R selectivity, and eventually got FDA approval in 2019 as Scenesse for a specific rare condition.
Meanwhile, MT-II went underground. Internet communities discovered the published research, started self-administering, and generated a flood of forum reports through the 2000s and 2010s. Several countries — UK, Australia, Norway — issued formal warnings or restricted sales. Five published melanoma cases and one renal infarction event sit in the medical literature, all linked to non-clinical Melanotan II use. The compound stayed in research circulation despite the regulatory friction because the published mechanism is genuinely interesting and because its specific receptor profile isn't replicated by any currently available alternative.
Here's the uncomfortable truth: Melanotan II has the worst safety signal of any compound currently sold as a research peptide. The melanoma cases in the literature are real. The renal infarction is real. The cardiovascular and dermatological adverse events documented in self-experimentation reports are real. Anyone selling MT-II as routinely safe is ignoring published case reports. The compound's pharmacology — non-selective melanocortin activation — is exactly what makes both its research interest and its risk profile distinct from cleaner pigmentation research tools.
For pigmentation research specifically, MT-II remains a useful pharmacological probe of melanocortin receptor signaling. For melanocortin receptor studies generally, the non-selectivity provides a different research tool than MC1R-selective agonists like afamelanotide. The compound has legitimate research uses. It also has documented case-report harms that other research peptides don't carry.
Regulatory note: Melanotan II was placed on the FDA's Category 2 bulks list in 2023. On April 22, 2026, the FDA removed Melanotan II from Category 2 after the original nominations were withdrawn. Unlike BPC-157, KPV, and others scheduled for July 2026 PCAC review, Melanotan II has been deferred to a PCAC consultation before the end of February 2027 — placing it in the second-tier reclassification group with weaker nomination support and stronger remaining safety concerns. As of May 2026, MT-II is in regulatory transition. WADA prohibits it for athletes in tested sports.
Here's a sourcing problem that's specific to Melanotan II: it's a cyclic peptide — the structure depends on a lactam bridge between specific residues that creates the ring conformation. That cyclization step is technically demanding during synthesis, and cheap production routinely delivers either linear (uncyclized) material or partially cyclized product mixed with linear contaminants. The linear form has dramatically reduced melanocortin receptor binding compared to the cyclic form. Without HPLC-MS verification specifically checking for ring closure, the defect is invisible and the compound that arrives at your bench may be the wrong molecular species entirely. Given the safety profile, sourcing reliability matters more here than for almost any other research peptide.
Generic Peptides supplies research-grade Melanotan II for sale at 99% purity, manufactured in the USA. Domestic synthesis with verified cyclization — the part that determines whether the molecule has the structure published research describes.
Order Melanotan II for sale in the USA — 99% purity, cyclic structure verified, manufactured domestically.
Yes — Melanotan II is legally available as a research compound in the United States. It was removed from FDA Category 2 on April 22, 2026, with PCAC consultation scheduled before the end of February 2027 (deferred to the second-tier review group rather than the July 2026 first-tier group). Not FDA-approved for human use. WADA prohibits it for tested athletes.
Different compounds, different selectivity profiles. Melanotan I (afamelanotide, brand name Scenesse) is FDA-approved for erythropoietic protoporphyria with cleaner MC1R selectivity. Melanotan II is a non-selective melanocortin receptor agonist that hits multiple receptor subtypes — primarily MC1R, MC3R, and MC4R — producing broader pharmacological effects but more side effects.
Because the published medical literature contains documented adverse events that other research peptides don't carry — five melanoma case reports and at least one renal infarction event linked to MT-II self-administration. The non-selective melanocortin activation produces effects on cardiovascular function, appetite, and skin biology that compound the risk profile. Honest assessment, not marketing language.
The non-selective receptor profile means MT-II also affects appetite (suppression via MC4R), sexual function (effects via MC4R), cardiovascular tone (modest blood pressure effects), and other melanocortin-dependent pathways. Research designs studying any single endpoint have to account for all the others. That breadth is part of what makes the compound mechanistically interesting and pharmacologically risky.
Probably not, and the difference matters more here than for most peptides. The cyclic structure requires specific synthesis steps that cheap production routinely skips, leaving you with linear (open-chain) material that doesn't bind melanocortin receptors properly. Given MT-II's narrow safety margin even when correctly synthesized, sourcing inconsistency adds another layer of risk on top of an already cautious-use compound.
Sources
Dorr RT et al. — "Evaluation of melanotan-II, a superpotent cyclic melanotropic peptide in a pilot phase-I clinical study." Life Sciences, 1996. Phase 1 trial confirming pharmacological activity in humans. https://pubmed.ncbi.nlm.nih.gov/8637402/
Peters B et al. — "Melanotan II: a possible cause of renal infarction: review of the literature and case report." CEN Case Reports, 2020. Documents the renal infarction case and reviews the melanoma literature. https://pubmed.ncbi.nlm.nih.gov/31953620/
Hadley ME, Dorr RT — "Melanocortin peptide therapeutics: historical milestones, clinical studies, and commercialization." Peptides, 2006. Comprehensive history of MT-II development at the University of Arizona. https://pubmed.ncbi.nlm.nih.gov/16934364/
FDA — "Bulk Drug Substances Nominated for Use in Compounding Under Section 503A," updated April 22, 2026. Documents Melanotan II removal from Category 2 and the deferred February 2027 PCAC consultation. https://www.fda.gov/media/94155/download
Cyclic structure. Non-selective receptor activity. Real safety signals in the literature. Sourcing isn't optional.
Melanotan II ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its cyclic heptapeptide structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24–36 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~12 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — Melanotan II contains a tryptophan residue that's particularly prone to photodegradation. | Always keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | The tryptophan and histidine residues make Melanotan II susceptible to oxidation if the vial seal is broken or the powder is exposed to air. | Keep the aluminum crimp cap intact until ready to reconstitute. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
Independent lab test reports are available for Melanotan II 5mg and 10mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

Non-selective melanocortin reference across MC1R through MC5R in our transfected panel. The pan-receptor activation profile is exactly what we use it for — the contrast against the selective agonists. Consistent.
Hruby and Hadley engineered this at Arizona back in the eighties as a photoprotection-research tool — that's the actual origin, long before the uses it later got associated with. Refreshing that the listing references the real development history. Material activated the receptor subtypes consistently in our panel.
We do melanocortin receptor crystallography and MT-II is a standard non-selective reference ligand for the structural work — characterizing how a pan-agonist sits in the binding pockets across subtypes. Material took our additional purification well and reached crystal grade. Useful that the listing carries it alongside the selective compounds for comparative structural studies.
Decent for our MC1R signaling characterization. Handling note: it's a cyclic heptapeptide, reasonably stable lyophilized, but I aliquot immediately and minimize freeze-thaw since cyclic conformation can be sensitive. Material was reliable across the working period. A cyclization-verification figure on the documentation would strengthen confidence, though.
What earned my trust was the listing actually acknowledging the documented adverse-event literature around this compound rather than glossing it — the case reports are substantial and a vendor that references them honestly is one I take more seriously for research procurement. Material itself behaved as expected in our receptor work.
For comparative melanocortin work, having the non-selective MT-II and the MC4R-selective bremelanotide from one source with matched documentation is the entire point — the selective-versus-non-selective contrast is the core experiment, and vendor variability would confound the receptor-selectivity readout. That single-source consistency is the real value here.
The relationship to bremelanotide is the elegant part — MT-II is the non-selective parent, and the single C-terminal change to the free acid gives you the MC4R-selective derivative. Studying them together illustrates how one modification reshapes receptor selectivity. Material consistent with that comparative framing.
Non-selective melanocortin reference for our receptor panel. Consistent batches, repeated orders. That's the review.
MT-II binds melanocortin-1 receptors (MC1R) on melanocytes — the pigment-producing cells in skin. Activation triggers the cAMP-PKA-MITF cascade that increases tyrosinase expression and stimulates eumelanin synthesis. The mechanism replicates what α-MSH does naturally during UV-induced tanning, but without requiring UV exposure to initiate the signaling.
Afamelanotide is more selective for MC1R, producing pigmentation effects with fewer off-target hormonal responses. Melanotan II is non-selective across multiple melanocortin receptors (MC1R, MC3R, MC4R, MC5R), producing broader pharmacological effects including appetite suppression and sexual function modulation. Afamelanotide reached FDA approval; MT-II didn't.
The non-selective melanocortin activation includes MC4R, which is heavily involved in appetite regulation and sexual response pathways in the central nervous system. MT-II's MC4R agonism produces measurable appetite suppression and effects on sexual desire that became part of the compound's research profile — and part of why it was difficult to develop as a clean pigmentation drug.
The cyclic peptide structure requires specific synthesis steps to form the lactam ring that defines its conformation. Cheap production routinely produces linear (uncyclized) material that lacks the proper three-dimensional structure for melanocortin receptor binding. HPLC-MS analysis specifically targeting cyclization is required to verify correct synthesis — most budget suppliers don't run this verification.
Melanotan II was developed in the 1980s and 1990s by researchers at the University of Arizona, led by Mac Hadley and Victor Hruby. The compound was originally pursued as a potential melanoma prevention agent — induced pigmentation might reduce UV-related skin cancer risk. The 1996 Dorr Phase 1 trial confirmed pharmacological activity in humans. Pharmaceutical development eventually shifted to the more selective afamelanotide.
Yes. WADA prohibits Melanotan II for athletes subject to drug testing. The compound's effects on appetite, body composition, and metabolic parameters place it in regulatory categories of concern for anti-doping authorities, and its non-selective melanocortin activity touches multiple physiological systems that other prohibited substances target.
MT-II, MT-2, Melanotan-2, and the chemical descriptor cyclic[Nle⁴, Asp⁵, D-Phe⁷, Lys¹⁰]-α-MSH(4-10). CAS number 121062-08-6. The cyclic heptapeptide structure is what defines the compound — different naming conventions across literature, all referring to the same cyclic structure.
Pigmentation research and melanocortin receptor pharmacology lead by volume — particularly comparative studies of selective vs non-selective melanocortin agonists. There's also active research in appetite regulation models (MC4R signaling), sexual function research, and erectile dysfunction pharmacology that emerged from MT-II's clinical development pipeline. Skin cancer prevention research has waned but isn't entirely absent from current literature.
PT-141 (Bremelanotide) is a metabolite of Melanotan II that retains MC4R activity but with a different selectivity profile. PT-141 was developed specifically for sexual function applications and reached FDA approval as Vyleesi for hypoactive sexual desire disorder in women. They share lineage but PT-141's selectivity makes it a different pharmacological tool with cleaner regulatory status.
Native α-MSH is a 13-amino-acid peptide that's biologically unstable, with a half-life measured in minutes and difficulty crossing physiological barriers. Melanotan II is a cyclic 7-amino-acid analog engineered for stability and potency — significantly more stable in circulation and more potent at melanocortin receptors. The trade-off is the non-selectivity that made it problematic as a clinical drug.
Researchers investigating melanocortin receptor pharmacology and non-selective MC receptor agonism consistently examine Melanotan II alongside compounds that target overlapping or complementary melanocortin pathways. PT-141 (Bremelanotide) is the most direct structural comparison — PT-141 is a metabolite of Melanotan II with the C-terminal amide group removed, which shifts receptor selectivity away from MC1R toward MC3R and MC4R; researchers studying the pharmacological consequences of that single structural modification often examine both compounds in parallel to isolate which receptor drives which effect. Kisspeptin-10 occasionally appears in the same reproductive neuroendocrinology research context — both compounds affect central signaling pathways relevant to sexual function, through completely different receptor systems, making them complementary tools for dissecting neurogenic vs HPG axis contributions to reproductive biology. Semax shares the broader melanocortin receptor family research space — Semax's ACTH-derived sequence has documented interactions with melanocortin receptors, and researchers studying MC receptor subtypes sometimes examine both compounds when mapping receptor-specific downstream effects. AOD 9604 appears in the same pigmentation and metabolic research context given overlapping interest in MC1R biology and fat metabolism pathways that both compounds touch through different mechanisms.