Thymosin Alpha-1 2mg
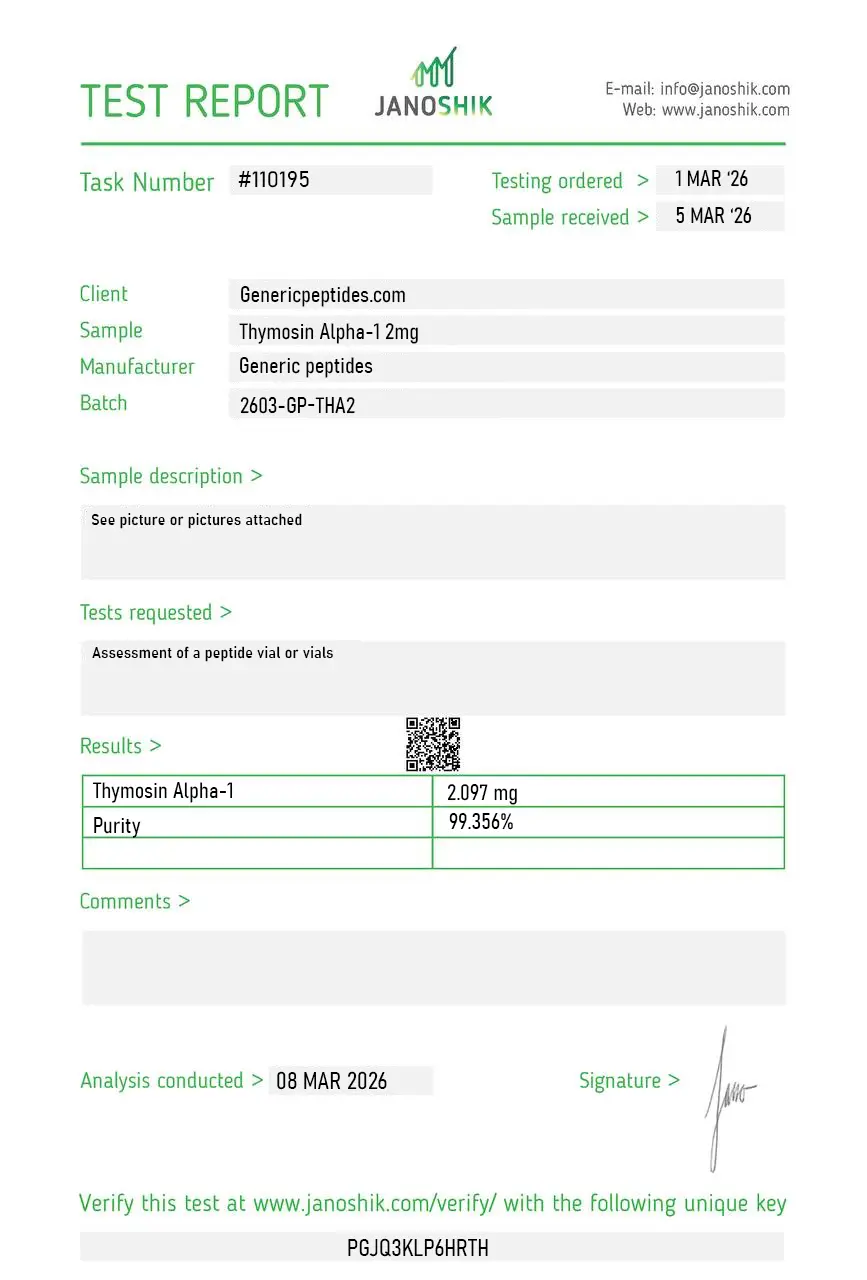
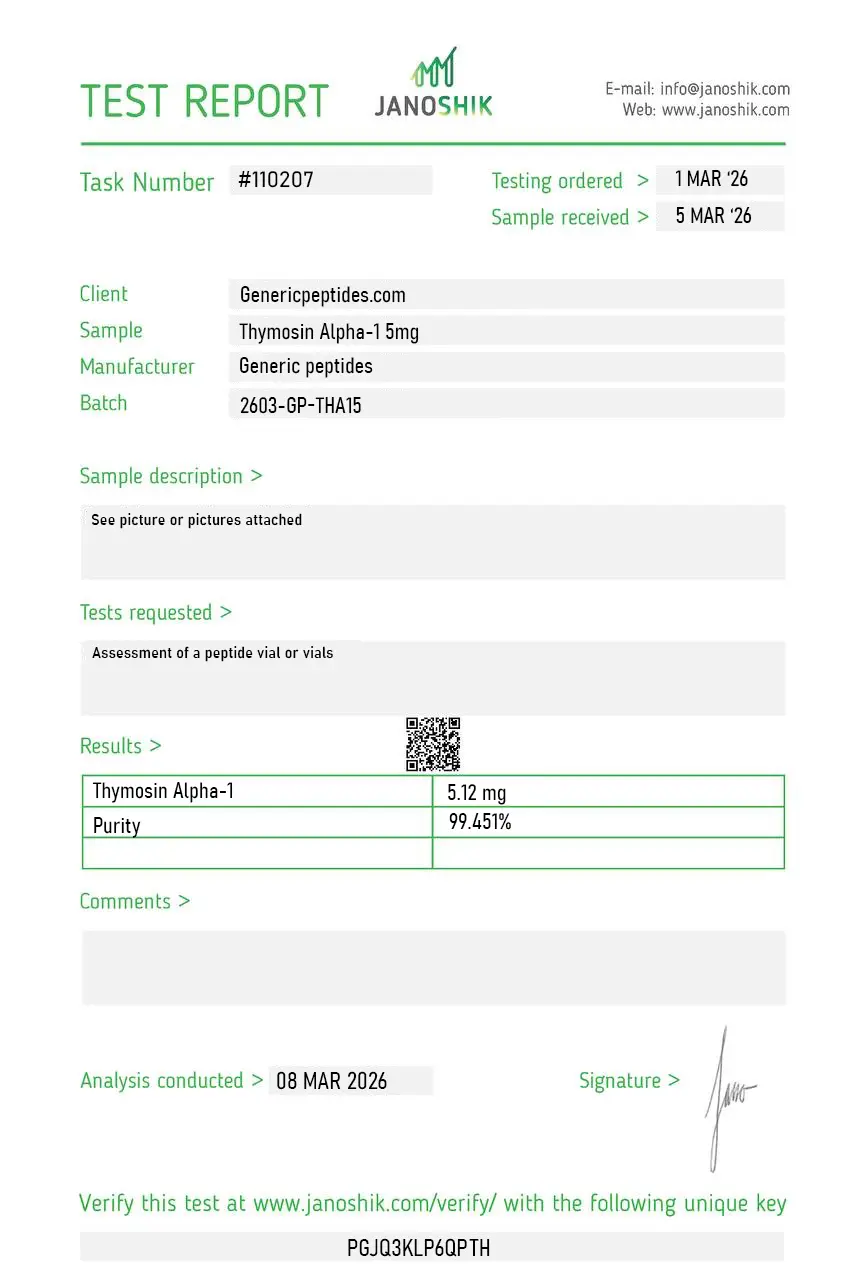
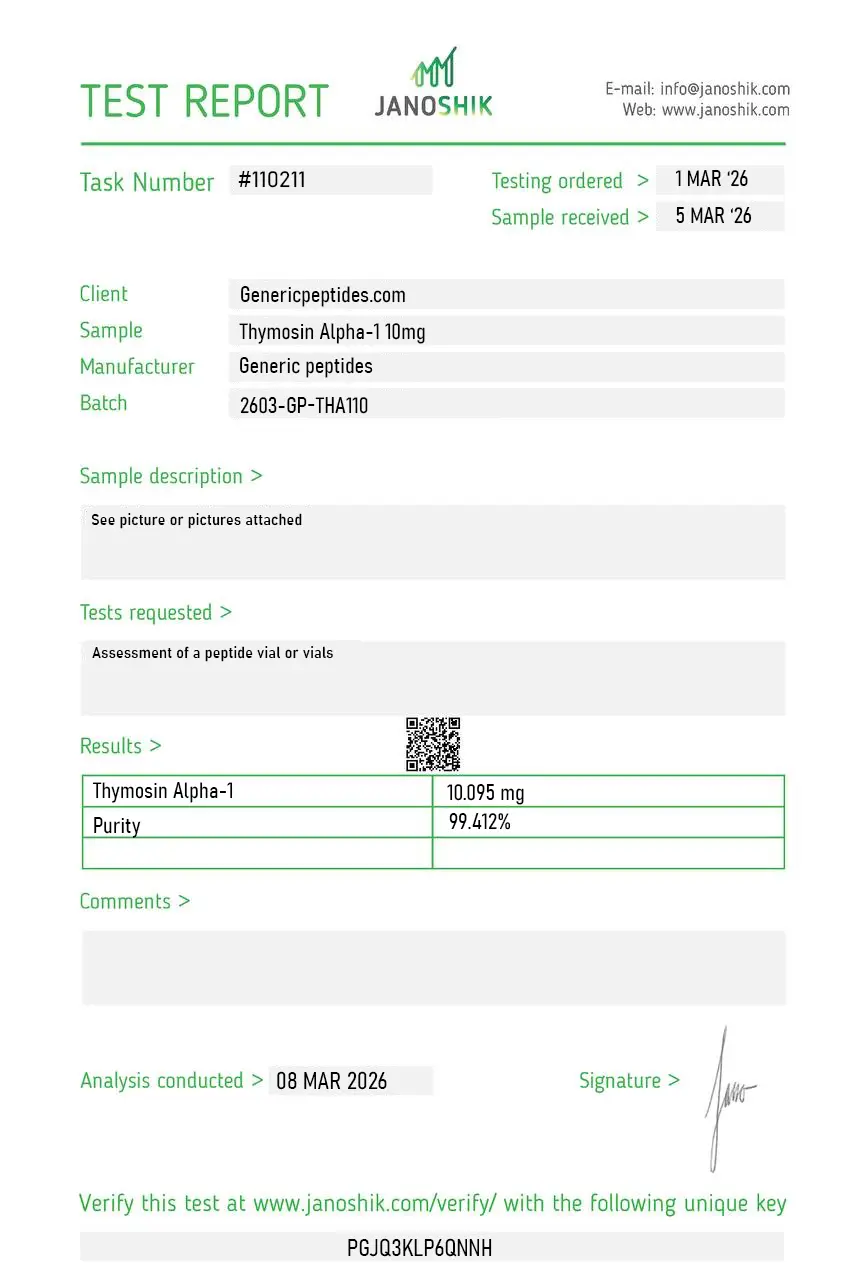
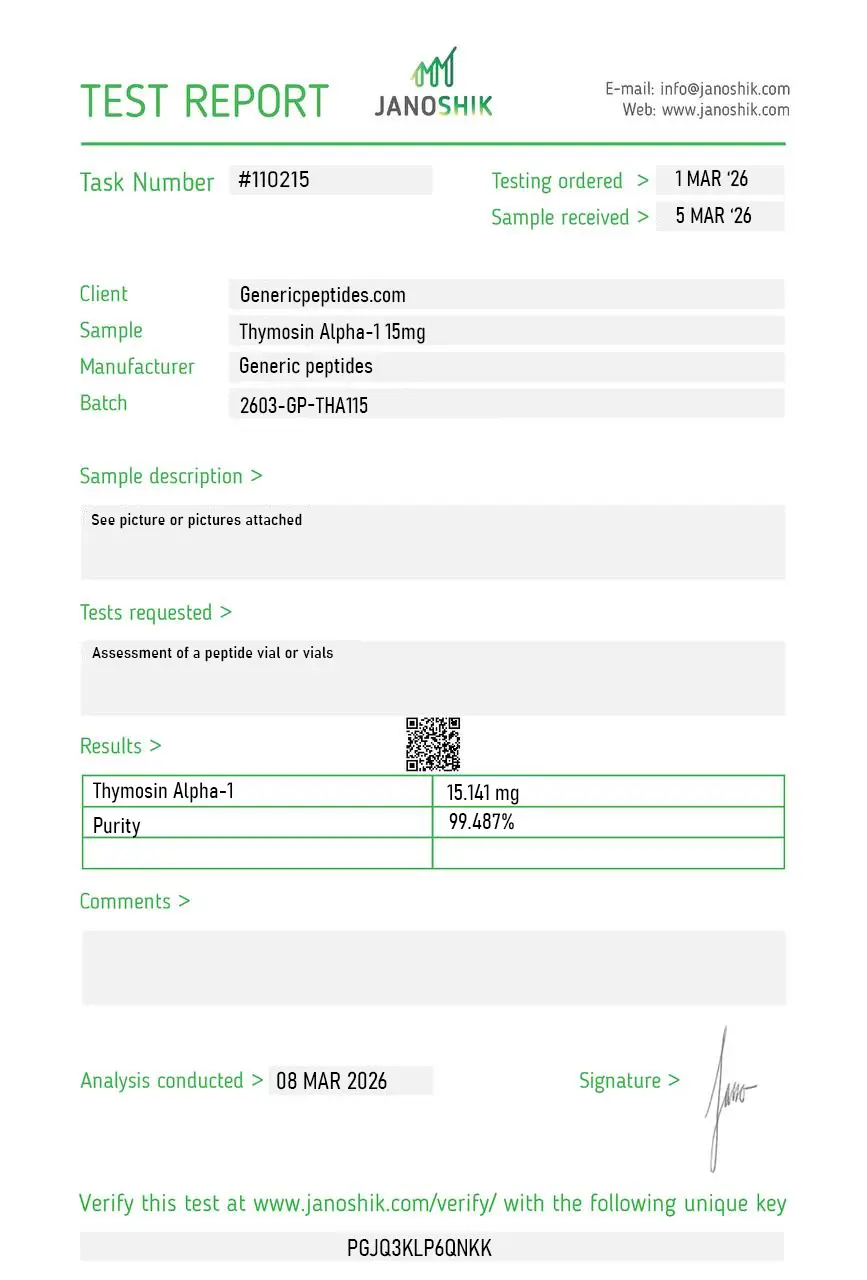
Certificate of Analysis available











Thymosin Alpha-1 is a prescription drug in over 35 countries — Italy, China, Cuba, and most of Southeast Asia. Italian doctors have been prescribing it since 1995 as Zadaxin for hepatitis B. Chinese hospitals administered it widely during the 2003 SARS outbreak. The 2020 COVID-19 research from Wuhan reported significant mortality reduction in severe cases. The one country where it's never been FDA-approved is the United States — and that's exactly why most American researchers had never heard of it before its 2023 placement on the FDA's restricted compounding list.
Thymosin Alpha-1 (Tα1) is a synthetic 28-amino-acid peptide with the sequence Ac-SDAAVDTSSEITTKDLKEKKEVVEEAEN. It's identical to a naturally occurring thymic peptide originally isolated from bovine thymus tissue by Allan Goldstein's research group at the George Washington University in 1977. The N-terminal acetylation is essential for biological activity — without it, the molecule loses most of its immunomodulatory function.
What makes Tα1 mechanistically distinct from most immunomodulators: it doesn't broadly stimulate or suppress the immune system. It acts as a balancer — through Toll-like Receptor activation on dendritic cells and macrophages — primarily TLR2 and TLR9 — which then orchestrates downstream effects on T-cell maturation, cytokine production, and CD4/CD8 ratios. The result is enhanced response to specific threats (viral infections, certain cancers) without the broad activation that drives autoimmunity. That selectivity is what made it commercially viable as a prescription drug across multiple countries.
Tα1's clinical research base is unusually deep for a peptide that's never been FDA-approved. The compound has been studied in over 70 published clinical trials covering hepatitis B and C (where it's an approved adjuvant therapy in multiple countries), HIV (where it's used as an immune modulator), severe sepsis, certain cancers, and most recently severe COVID-19. The 2020 Wuhan COVID-19 study showed Tα1-treated severe COVID-19 patients had significantly reduced mortality compared to controls, with the effect appearing strongest in patients with severe lymphopenia.
So why no FDA approval? Mostly economics. SciClone Pharmaceuticals, the original developer, focused regulatory efforts in markets where hepatitis B prevalence justified the development cost — China particularly. The US market for hepatitis B-specific therapy was smaller, more crowded with alternative treatments, and the regulatory bar higher. The compound passed FDA Phase 2 trials in hepatitis C but Phase 3 results in HCV monotherapy were inconclusive. Combined with the FDA's regulatory shift to combination antiviral therapies, the commercial path narrowed. The clinical evidence didn't disappear; the regulatory pathway just diverged from US approval.
Here's the honest part: Tα1's regulatory status in the US has been chaotic. The compound was placed on the FDA's Category 2 bulks list in September 2023, removed from Category 2 in September 2024 (alongside CJC-1295, Ipamorelin, Selank, and AOD-9604) when the original nominations were withdrawn, then reviewed by the PCAC at its December 4, 2024 meeting where the committee voted against Category 1 inclusion. As of May 2026, Tα1 is in regulatory limbo — not in Category 2, not in Category 1, not eligible for 503A compounding pharmacy production.
The international FDA-approved-elsewhere status doesn't translate to US compounding eligibility. The 503A statutory criteria require US-specific drug component status, USP/NF monograph, or 503A bulks list inclusion — international regulatory approval doesn't qualify. So while Tα1 is a regulated medicinal product in 35+ countries, in the US it sits in a research-compound-only channel pending resolution of the 503A status question.
Sales as a research compound continue legally in the US for laboratory use. WADA's Prohibited List does not specifically name Thymosin Alpha-1 as of 2025.
Here's a sourcing problem that's specific to Tα1: the N-terminal acetylation is essential for biological activity, and cheap synthesis routinely produces under-acetylated material that's structurally close to Tα1 but pharmacologically substantially weaker. The 28-amino-acid sequence alone isn't fully active — the acetyl group at the N-terminus is part of what defines the compound's interaction with TLR9 and the dendritic cell signaling cascade. Without HPLC-MS verification specifically targeting the acetylation, you may have material that's labeled correctly, has the right molecular weight within tolerance, but doesn't behave like the Zadaxin-grade Tα1 that 35+ countries have approved as a prescription medication.
Generic Peptides supplies research-grade Thymosin Alpha-1 for sale at 99% purity, manufactured in the USA. Domestic synthesis with verified N-terminal acetylation — the part that determines whether your Tα1 actually has the structural integrity that decades of international clinical research describes.
Order Thymosin Alpha-1 for sale in the USA — 99% purity, verified N-terminal acetylation, manufactured domestically.
Yes — Thymosin Alpha-1 is legally available as a research compound in the United States. It was removed from FDA Category 2 in September 2024 and reviewed by the PCAC in December 2024, but was not added to the Category 1 bulks list. As of May 2026, it sits in regulatory transition. It's not FDA-approved for human use in the US, though it's an approved prescription drug in over 35 other countries as Zadaxin.
Different compounds with overlapping research applications. Thymosin Alpha-1 is a single defined 28-amino-acid synthesized peptide originally isolated by Goldstein's group in the West, with substantial international regulatory approval (Zadaxin in 35+ countries). Thymalin is a Russian polypeptide complex (mixture) extracted from calf thymus, with KE, EW, and EDP as principal active components. Different molecules, different research traditions.
Mostly economic and regulatory pathway reasons. SciClone Pharmaceuticals, the original developer, focused approval efforts in markets with high hepatitis B prevalence — China particularly. US Phase 3 trials in HCV monotherapy were inconclusive, and the FDA's shift to combination antiviral therapies narrowed the commercial path. The clinical evidence is real; the US regulatory pathway diverged from international approvals.
Yes — Zadaxin is the brand name under which Thymosin Alpha-1 is marketed in countries where it's approved (Italy, China, Cuba, etc.). The compound is also called thymalfasin (the INN), Tα1, ZADAXIN, and various commercial designations. CAS number 62304-98-7. The 28-amino-acid sequence with N-terminal acetylation identifies the molecule unambiguously.
Probably not at the same purity or with intact acetylation. The N-terminal acetylation is essential for biological activity, and cheap synthesis routinely delivers under-acetylated material that's pharmacologically substantially weaker than the Zadaxin-grade compound. Without HPLC-MS verification of acetylation status, the difference is invisible until your TLR9 binding assay produces inconsistent results.
Sources
Liu Y, Pan Y, Hu Z et al. — "Thymosin Alpha 1 Reduces the Mortality of Severe Coronavirus Disease 2019 by Restoration of Lymphocytopenia and Reversion of Exhausted T Cells." Clinical Infectious Diseases, 2020. The Wuhan COVID-19 mortality reduction study. https://pubmed.ncbi.nlm.nih.gov/32442287/
Goldstein AL, Badamchian M — "Thymosins: chemistry and biological properties in health and disease." Expert Opinion on Biological Therapy, 2004. Comprehensive review by the discovery group, documenting the 1977 isolation and clinical applications. https://pubmed.ncbi.nlm.nih.gov/15268670/
Camerini R, Garaci E — "Historical review of thymosin alpha 1 in infectious diseases." Expert Opinion on Biological Therapy, 2015. Documents the international regulatory approval pathway and clinical trial history across hepatitis B/C, HIV, and cancer applications. https://pubmed.ncbi.nlm.nih.gov/25831172/
FDA — "Bulk Drug Substances Nominated for Use in Compounding Under Section 503A," updated April 22, 2026. Documents Thymosin Alpha-1 acetate and free base removal from Category 2 (September 2024) and the December 2024 PCAC review. https://www.fda.gov/media/94155/download
Approved in 35+ countries. Not approved in one. The acetylation is the entire molecule.
Thymosin Alpha-1 ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its 28-amino-acid acetylated structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — protect from direct light and UV exposure to prevent photodegradation. | Keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, clumping, visible moisture, or a sticky texture — the acidic and basic residues in Tα1 can attract humidity if the seal is broken. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
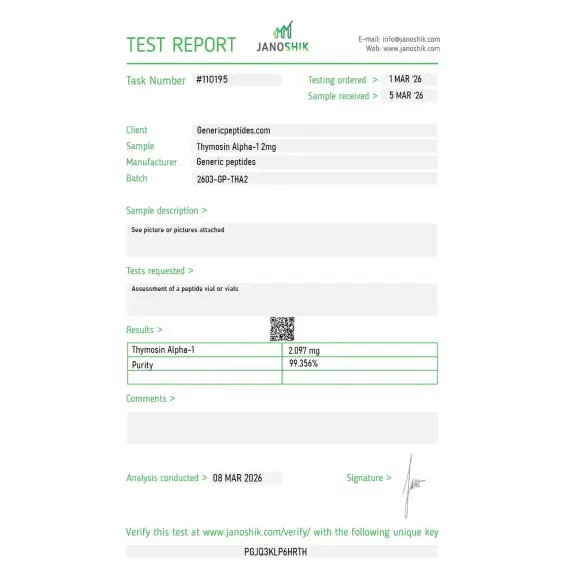
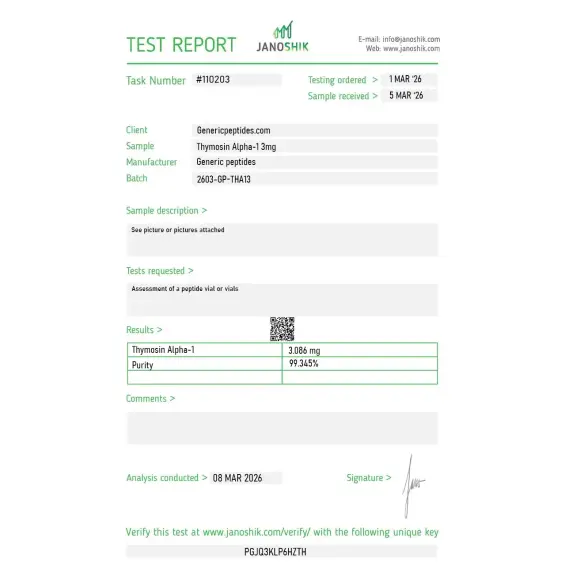
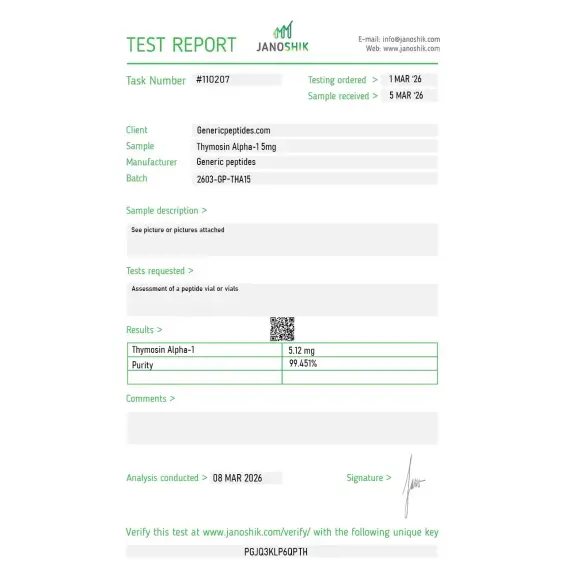
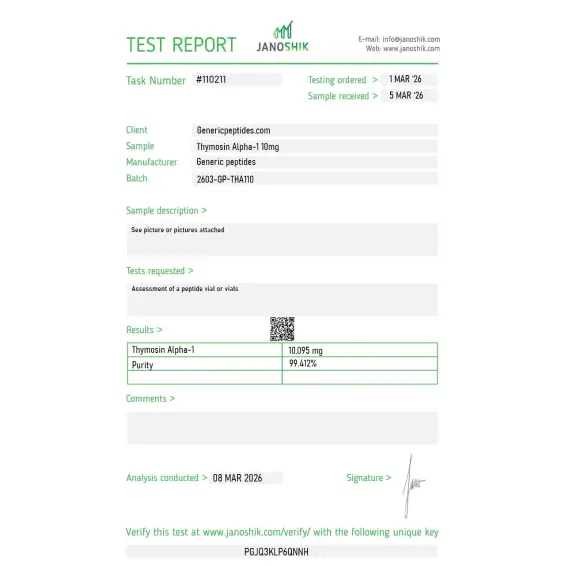
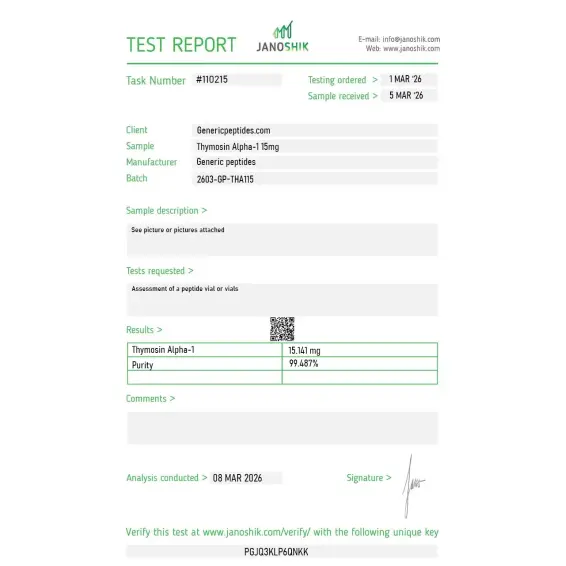
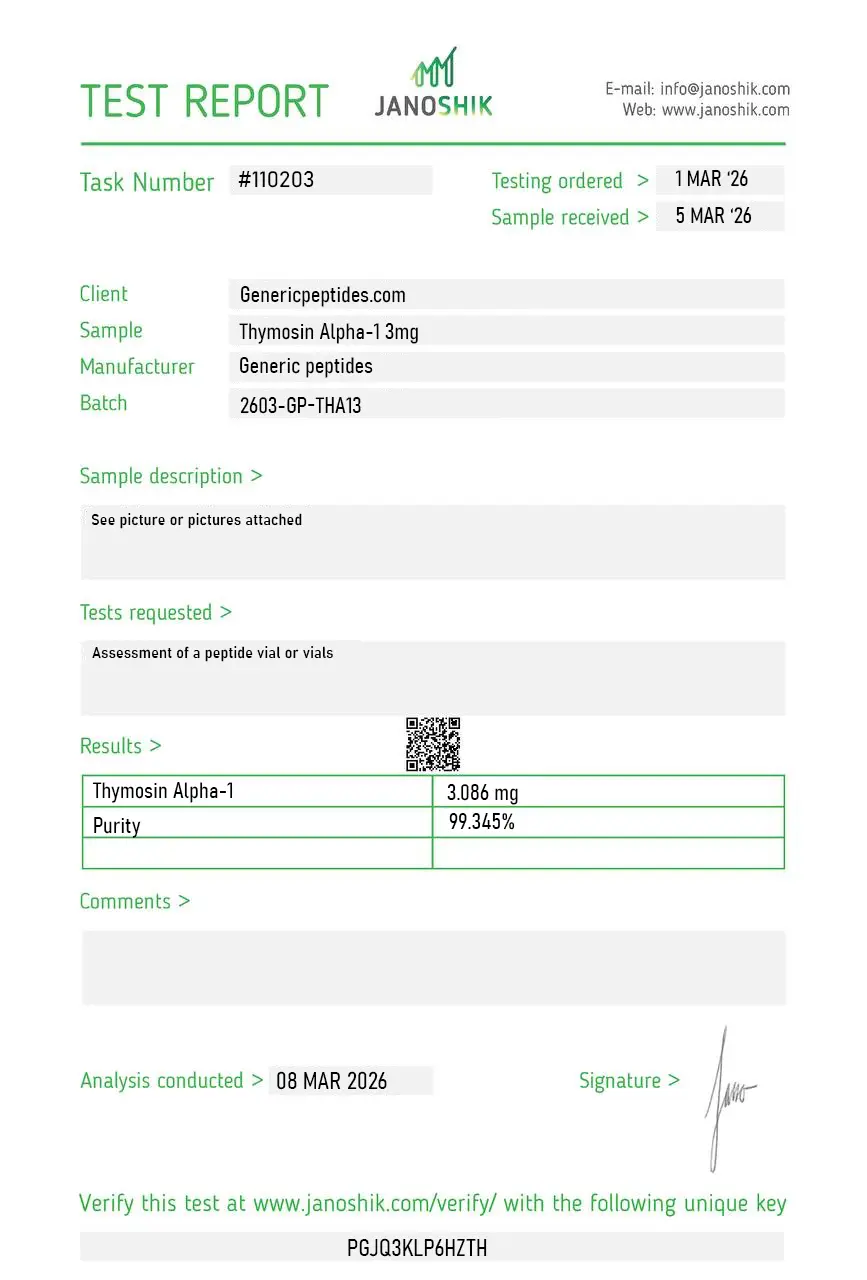
Independent lab test reports are available for Thymosin Alpha-1 2mg, 3mg, 5mg, 10mg, and 15mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.
TLR9 signaling in dendritic cells. Did what it should.
Goldstein's original thymosin fraction work is genuinely foundational immunology and it's refreshing that the listing treats this as the characterized synthetic peptide it is. Material gave consistent results in our innate-immune signaling assays.
The single most important thing about ordering this is making sure you're getting Thymosin Alpha-1 and not Thymalin — the Russian thymic extract. They're constantly conflated and they're completely different products, one a defined synthetic 28-mer, the other an undefined polypeptide mixture. This vendor distinguishes them, which is why I ordered here. Knocking a star only because the N-terminal acetylation wasn't explicitly confirmed on the COA and for this peptide that modification matters.
Acetylation confirmed by mass spec on the COA, which is the one thing I always check for this peptide — the unmodified form has measurably different activity and not every supplier verifies it. Good documentation.
Reorder for ongoing dendritic-cell maturation work. Consistent.
What I needed was the defined synthetic, not the Russian extract, for an experiment where I had to know exactly what molecule I was adding. Twenty-eight residues, known sequence, acetylated N-terminus. That precision is the entire reason synthetic Thymosin Alpha-1 exists as distinct from the older thymic preparations.
The approval status of this peptide is genuinely confusing — approved in something like thirty-five countries for hepatitis indications, not FDA-approved, and the listing actually acknowledges that complexity rather than implying blanket approval or blanket prohibition. For procurement justification that nuance is useful.
Tα1 binds Toll-like Receptor 9 (TLR9) on dendritic cells and macrophages, triggering downstream signaling that orchestrates T-cell maturation, cytokine production, and CD4/CD8 ratio normalization. The mechanism is selective rather than broadly stimulatory — it enhances response to specific threats without triggering broad immune activation. That balanced effect is mechanistically distinct from purely immunostimulant compounds.
Different molecules with different mechanisms despite the shared "thymosin" name. Tα1 is a 28-amino-acid immunomodulator targeting TLR9 and T-cell function. Tβ4 (TB-500) is a 43-amino-acid actin-sequestering peptide affecting cell migration and tissue repair. Different families, different research applications, different regulatory pathways. The "thymosin" label reflects historical isolation from thymus tissue rather than functional similarity.
Pure immunostimulants broadly activate immune function, which carries autoimmunity risk and side effects. Tα1 selectively enhances appropriate immune responses through TLR9-mediated dendritic cell signaling without producing broad activation. The published clinical evidence supports better outcomes in conditions of immune dysregulation (hepatitis B, severe sepsis, COVID-19) without the autoimmune complications of broader stimulants.
The N-terminal acetylation is essential for full biological activity, and cheap synthesis routinely produces under-acetylated material with significantly reduced TLR9 binding. The 28-amino-acid sequence has multiple synthesis-vulnerable positions including the acidic residues that need careful protection during peptide chain extension. Detection of acetylation defects requires HPLC-MS analysis specifically targeting the modification.
Thymosin Alpha-1 was isolated and characterized by Allan Goldstein and colleagues at the Albert Einstein College of Medicine in 1977, originally extracted from bovine thymus tissue. The first commercial approval came in Italy (Zadaxin for hepatitis B) in 1995, with subsequent approvals expanding to over 35 countries. The compound has approximately five decades of research and clinical history.
Thymosin Alpha-1 is not specifically named on the WADA Prohibited List as of 2025. Tα1's mechanism — selective immunomodulation through TLR9 signaling — doesn't fit standard performance-enhancing categories. Athletes subject to drug testing should consult their governing body's specific rules — anti-doping rules can include unspecified substances under broad immunomodulator categories.
Thymalfasin (the INN), Zadaxin (the international brand name from SciClone), Tα1, Ta1, Talpha1, and the chemical sequence Ac-SDAAVDTSSEITTKDLKEKKEVVEEAEN. CAS number 62304-98-7. Different naming conventions across literature reflecting whether the source is research, clinical, or commercial.
Hepatitis B and C research lead by clinical volume — particularly in countries where Tα1 is an approved adjuvant therapy. HIV immune restoration research has continued for decades. The most recent research expansion was severe COVID-19, where the 2020 Wuhan study and subsequent work demonstrated mortality reduction in severe cases. Cancer immunotherapy (particularly melanoma adjuvant), severe sepsis, and immune restoration after chemotherapy are additional active research areas.
Different mechanisms, complementary applications. Interferons are larger proteins that broadly activate antiviral responses across multiple cell types with significant side effect profiles. Tα1 acts more selectively through TLR9-mediated dendritic cell signaling with substantially fewer side effects. Clinical research has investigated both as monotherapy and in combination — Tα1 sometimes enhances interferon efficacy in hepatitis treatment protocols.
Most research-stage immunomodulator peptides have limited clinical validation. Thymosin Alpha-1 is unusual in having extensive international regulatory approval (35+ countries), 50+ years of research history, 70+ published clinical trials, and continuous medicinal use in established healthcare systems. The US regulatory gap is the exception rather than the rule for this compound — the international clinical and research base is substantially deeper than for most peptides currently sold in the research market.
Researchers investigating thymic immune modulation, TLR-mediated innate immunity, and immunosenescence consistently examine Thymosin Alpha-1 alongside compounds that target overlapping or complementary aspects of immune function and anti-aging biology. Thymalin is the most natural pairing — both are thymus-derived immune modulators, but Thymosin Alpha-1 is a single defined 28-amino-acid Western-characterized peptide while Thymalin is a Russian polypeptide complex; researchers comparing defined vs mixture-based thymic preparations, or studying comprehensive thymic immune restoration, examine both to map the contribution of specific peptide components vs the full extract. Epitalon shares the anti-aging immune research space — both appear in the Russian bioregulator literature studying longevity, and researchers examining the relationship between immune senescence and telomere biology sometimes examine both simultaneously to address thymic and pineal contributions to aging biology. BPC-157 occasionally appears in the same immune modulation and gut health research context — both compounds affect inflammatory signaling and immune cell function, and researchers studying the gut-immune axis sometimes examine both given Thymosin Alpha-1's documented effects on gut-associated lymphoid tissue. NAD+ addresses immune cell metabolism through mitochondrial function and sirtuin activation — a complementary metabolic approach to Thymosin Alpha-1's receptor-mediated immune modulation for researchers studying comprehensive immune aging biology. PNC-27 appears in the same cancer immunology research context given both compounds' documented effects on tumor immune responses and their shared research base in oncology-focused peptide pharmacology.