MET-5 20mg
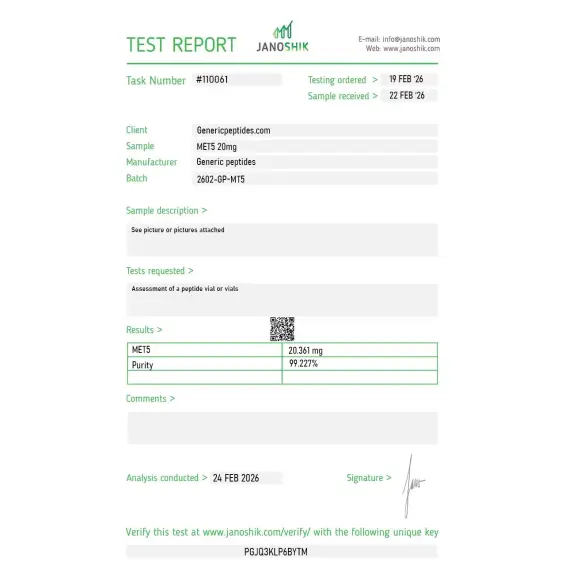
Certificate of Analysis available




In 1975, John Hughes and Hans Kosterlitz at the University of Aberdeen published a finding that rewrote pharmacology textbooks: the brain produces its own opioids. They isolated two pentapeptides from pig brain extract that bound the same receptors as morphine. One ended in methionine. One ended in leucine. Together they're called the enkephalins — and they were the first endogenous opioids ever identified. MET5 is the methionine version.
MET5 is the research designation for Methionine-Enkephalin (Met-Enkephalin or Met-Enk) — a naturally occurring 5-amino-acid neuropeptide with the sequence Tyr-Gly-Gly-Phe-Met. The "5" refers to the methionine residue at position 5, which distinguishes it from leucine-enkephalin (the other enkephalin variant). The compound is endogenously produced in the central nervous system, the adrenal medulla, and throughout the spinal cord, derived from larger precursor proteins like proenkephalin.
Its primary mechanism is agonism at the delta-opioid receptor (DOR), with secondary activity at the mu-opioid receptor and minimal kappa receptor binding. The tyrosine residue at position 1 is structurally analogous to the 3-hydroxyl group on morphine — that's the part that lets the molecule fit the opioid receptor pocket. Without that conserved tyrosine, the molecule loses its opioid activity entirely.
MET5 serves two largely separate research literatures. The first and oldest is opioid pharmacology — pain perception, stress response, gastrointestinal motility, and reward circuit research. As the prototypical endogenous delta-opioid agonist, MET5 is a reference compound for any study investigating DOR signaling, opioid receptor desensitization, or comparison with synthetic opioid analogs.
The second research identity emerged in the 1980s. Researchers discovered that Met-enkephalin regulates cell proliferation in normal and neoplastic cell lines through a distinct receptor — the OGF receptor (OGFr), which is structurally and molecularly different from the classical mu/delta/kappa opioid receptors. In this context, the same molecule is called Opioid Growth Factor, and it has its own research literature investigating cancer cell biology, wound healing, and tissue regeneration. Same pentapeptide, two completely different receptor systems, two different research communities.
Here's the uncomfortable truth: MET5 has a ~minutes-long biological half-life in plasma due to rapid degradation by enkephalinases and aminopeptidases. The molecule is cleaved at the Tyr-Gly bond almost immediately after release. That instability is the primary reason it never became a clinical drug — you'd need to administer doses multiple times an hour to maintain therapeutic concentrations. For research, this rapid metabolism is sometimes a feature (controlled, time-limited DOR activation) and sometimes a fundamental limitation (any study requiring sustained exposure). Researchers either work around it with continuous infusion or use stabilized analogs like DAMGO or DPDPE that resist enzymatic cleavage.
Regulatory note: MET5 / Met-Enkephalin is not on the FDA's 503A bulks list. It wasn't part of the recent Category 2 reclassification activity affecting BPC-157, Epitalon, DSIP, and others — it occupies a different regulatory category as an endogenous opioid peptide rather than a synthetic novel pharmaceutical. As a research compound, it remains commercially available in the United States. Athletes subject to drug testing should consult their governing body's specific rules — endogenous opioid peptides occupy nuanced regulatory territory.
Here's a sourcing problem that's specific to MET5: the methionine residue at position 5 is vulnerable to oxidation during synthesis and storage. Oxidized methionine (methionine sulfoxide) changes the receptor binding profile significantly — and the visible appearance of the peptide doesn't change. Cheap synthesis routes and improper storage routinely produce material with partial methionine oxidation, giving you a compound that's structurally close to MET5 but pharmacologically different. Without analytical verification specifically checking for methionine oxidation state, this defect is invisible to buyers and ruins any study where receptor binding affinity matters.
Generic Peptides supplies research-grade MET5 for sale at 99% purity, manufactured in the USA. Domestic synthesis with methionine integrity verified — the part that determines whether the compound behaves like the endogenous Met-Enkephalin published research describes.
Order MET5 for sale in the USA — 99% purity, full Tyr-Gly-Gly-Phe-Met sequence, manufactured domestically.
Yes — MET5 / Met-Enkephalin is legally available as a research compound in the United States. It's not on the FDA's 503A bulks list and wasn't part of the recent Category 2 reclassification activity. It's an endogenous opioid peptide, not a synthetic novel pharmaceutical, which places it in a different regulatory category from most of the peptides currently in regulatory transition.
They're the same compound. MET5 is the research designation referencing the methionine residue at position 5 of the pentapeptide. Met-Enkephalin is the full chemical name. You'll also see the molecule called Met-Enk, methionine-enkephalin, or — in cancer/cell proliferation research — Opioid Growth Factor (OGF). All four names refer to Tyr-Gly-Gly-Phe-Met.
OGF is the alternate name for Met-Enkephalin in cell proliferation research. The molecule binds a distinct receptor (OGFr) that's structurally different from the classical mu/delta/kappa opioid receptors. OGFr signaling regulates cell proliferation rather than pain perception. Same MET5 molecule, different receptor, different research literature — particularly active in oncology and wound healing studies.
The pentapeptide is rapidly cleaved by enkephalinases and aminopeptidases at the Tyr-Gly bond, with biological half-life measured in minutes. Researchers either use continuous infusion to maintain steady-state concentrations or substitute stabilized analogs (DAMGO for mu-receptor work, DPDPE for delta-receptor work) when sustained exposure is needed. The instability is also why MET5 never became a clinical pharmaceutical.
Probably not at the same purity or methionine integrity. The methionine residue oxidizes easily during synthesis and storage, producing material that looks correct on a label but behaves differently in receptor binding studies. Cheap suppliers don't typically run the analytical verification needed to confirm that the methionine hasn't been oxidized to methionine sulfoxide.
Sources
Hughes J, Smith TW, Kosterlitz HW et al. — "Identification of two related pentapeptides from the brain with potent opiate agonist activity." Nature, 1975. The foundational discovery paper for met- and leu-enkephalin. https://pubmed.ncbi.nlm.nih.gov/1207728/
Akil H et al. — "Endogenous opioids: biology and function." Annual Review of Neuroscience, 1984. Comprehensive review of enkephalin precursor proteins (proenkephalin, prodynorphin, POMC). https://pubmed.ncbi.nlm.nih.gov/6324644/
"Physiology, Enkephalin." StatPearls / NCBI Bookshelf. Documents the OGF receptor and dual research identity of Met-Enkephalin. https://www.ncbi.nlm.nih.gov/books/NBK557764/
"Met-Enkephalin." ScienceDirect Topics — Documents delta and mu opioid receptor selectivity, half-life characteristics, and research applications. https://www.sciencedirect.com/topics/neuroscience/met-enkephalin
The first endogenous opioid ever discovered. Methionine integrity is the entire molecule.
Met-enkephalin ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its 5-amino-acid opioid peptide structure (Tyr-Gly-Gly-Phe-Met) and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — Met-enkephalin contains tyrosine and methionine residues that are prone to photodegradation. | Always keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | The methionine residue is highly oxidation-prone (converting to methionine sulfoxide on air exposure), making a tight seal essential. | Keep the aluminum crimp cap intact until ready to reconstitute. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
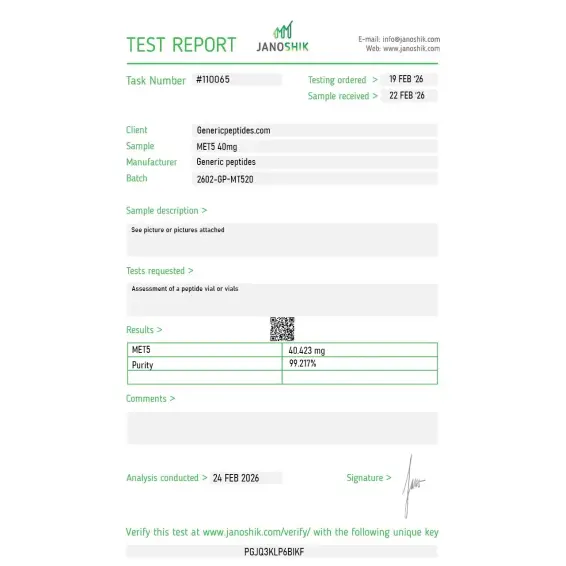
Independent lab test reports are available for MET-5 20mg and 40mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

δ-opioid receptor binding in transfected lines. The DOR-preference over MOR that distinguishes Met- from Leu-enkephalin came through as the literature describes. Consistent.
Hughes and Kosterlitz isolating this from brain in 1975 is genuinely one of the landmark discoveries in opioid pharmacology — it opened the whole endogenous-opioid field. Nice that the listing treats Met-enkephalin as the foundational ligand it is. Material gave clean displacement curves in our radioligand work.
The Penn State / Plotnikoff historical context on the product page is the kind of detail that distinguishes the listing from generic vendor descriptions. The 1980s-1990s immunomodulation research from Plotnikoff's group at Pennsylvania State established many of the foundational findings for enkephalin biology beyond pain — anti-tumor immunity, immune cell modulation, HIV adjunct research. Most current catalogs treat MENK only as an opioid receptor reference compound and miss the immunology context entirely.
The Shan group's modern cancer-immunology work at China Medical University is what makes this still a live research compound rather than a 1970s relic — macrophage polarization, dendritic-cell maturation, that direction. The listing referencing the immunomodulation angle, not just the opioid pharmacology, is why I trusted it for our immune work. Material consistent.
Reliable in our radioligand displacement work. Reconstituted cleanly. Practical note: we aliquot and store at minus-eighty under argon specifically because of the Met oxidation risk — more fuss than a typical pentapeptide needs, but it preserves activity. Material held up under that protocol. Worth the extra handling step for a Met-containing sequence.
We run Met- and Leu-enkephalin side by side to characterize the DOR-versus-MOR selectivity difference that the single C-terminal residue produces — methionine versus leucine, otherwise identical pentapeptides. Sourcing both from one place keeps the comparison clean. That one-residue selectivity contrast is the actual experiment.
MET5 binds primarily to the delta-opioid receptor (DOR) and secondarily to the mu-opioid receptor, both G-protein-coupled receptors. Activation triggers Gi/o signaling that inhibits adenylyl cyclase, reduces cAMP production, opens potassium channels, and closes voltage-gated calcium channels. The downstream effects include reduced neuronal excitability and decreased neurotransmitter release — the same pathway morphine uses, just at different receptor subtype affinities.
The carboxy-terminal amino acid: methionine in MET5, leucine in Leu-Enkephalin. The first four residues (Tyr-Gly-Gly-Phe) are identical. Both are pentapeptide endogenous opioids with similar receptor selectivity profiles, though MET5 generally shows slightly higher affinity at delta and mu receptors. Both are derived from the proenkephalin precursor protein.
Researchers in the 1980s discovered that Met-Enkephalin regulates cell proliferation through a distinct receptor (OGFr) that's structurally different from classical opioid receptors. In cell proliferation and oncology research, the molecule is called OGF rather than Met-Enkephalin. Same compound, different receptor, different research community — the dual naming reflects the parallel research identities.
The methionine residue at position 5 oxidizes easily during synthesis and storage, producing methionine sulfoxide that has altered receptor binding. The peptide looks identical on a label but behaves differently in binding assays. Cheap synthesis frequently delivers partially oxidized material, and most budget suppliers don't run the analytical verification needed to confirm methionine integrity.
Met-Enkephalin was discovered and characterized by John Hughes and Hans Kosterlitz at the University of Aberdeen in 1975, alongside Leu-Enkephalin. The discovery was foundational — these were the first endogenous opioid peptides ever identified, opening the entire field of endogenous opioid research. The 1975 Nature paper remains one of the most-cited papers in neuropharmacology.
Athletes subject to drug testing should consult their governing body's specific rules. As an endogenous opioid peptide, MET5 occupies regulatory territory different from synthetic opioids and from anabolic peptides. WADA's prohibited list includes various opioid-related categories that may apply depending on context and intended use.
Met-Enkephalin, Met-Enk, methionine-enkephalin, metenkefalin (the INN), Opioid Growth Factor (OGF), and the chemical sequence YGGFM (single-letter codes). CAS number 58569-55-4. Different naming conventions across literatures depending on whether the focus is opioid pharmacology or cell proliferation research.
Opioid receptor pharmacology and pain modulation research lead historical volume — MET5 is the prototypical endogenous delta-opioid agonist, used as a reference compound in countless DOR studies. Cell proliferation and cancer research (under the OGF designation) has been a parallel research thread since the 1980s. Stress response biology, gastrointestinal motility research, and immune modulation are additional active research areas.
DAMGO ([D-Ala²,N-MePhe⁴,Gly-ol]-enkephalin) is a synthetic enkephalin analog engineered for stability and mu-opioid receptor selectivity. MET5 is the natural endogenous peptide with rapid enzymatic degradation and broader delta/mu activity. DAMGO is used when researchers need stable, mu-selective binding; MET5 is used when natural enkephalin pharmacology is the experimental target.
MET5 was the first endogenous opioid ever discovered, alongside Leu-Enkephalin. Beta-endorphin (a longer 31-amino-acid peptide) and dynorphin (variable lengths) followed. Among endogenous opioids, the enkephalins are uniquely small and uniquely fast-acting — short half-lives, rapid receptor turnover, distributed throughout multiple brain regions. That brevity and ubiquity makes them mechanistically distinct from the longer, more sustained endorphin and dynorphin systems.
Researchers investigating endogenous opioid pharmacology, delta-opioid receptor signaling, and the OGF/OGFr cell proliferation axis consistently examine MET5 alongside compounds that target overlapping or complementary neurological and immunomodulatory pathways. Selank is a natural complement — both are short peptides with documented effects on enkephalin processing and GABAergic signaling, and Selank's mechanism explicitly includes modulation of enkephalin degradation pathways that directly affect endogenous MET5 activity; researchers studying the relationship between opioid tone and anxiety often examine both simultaneously. Semax shares the broader neuropeptide research space — both are studied in cognitive and stress response contexts, and Semax's documented effects on dopaminergic and serotonergic systems interact with the opioid circuits that MET5 modulates. DSIP addresses sleep architecture and stress response through a different neuropeptide mechanism — researchers studying the neurochemical basis of stress resilience and pain modulation sometimes examine all three Russian-origin neuropeptides together to map overlapping CNS pathways. Thymosin Alpha-1 occasionally appears in the same OGF/cell proliferation research context given both compounds' documented effects on immune cell function and their intersection in cancer biology research where the OGFr axis is most actively studied.