DSIP 2mg
Certificate of Analysis available




Swiss researchers electrically induced sleep in rabbits, then drew blood from their brains to find out what molecule was telling the rest of the body to sleep too. They found one. It was a 9-amino-acid peptide that did something most sleep compounds can't: it pushed brain activity into delta-wave (deep) sleep without sedating anything. That was 1977. The compound is DSIP, and the mystery of how it actually works is still mostly unsolved.
DSIP stands for Delta Sleep-Inducing Peptide. It's a tiny 9-amino-acid neuropeptide with the sequence Trp-Ala-Gly-Gly-Asp-Ala-Ser-Gly-Glu (WAGGDASGE). The FDA's official name for it is Emideltide. It was first isolated in 1977 by Schoenenberger and Monnier at the University of Basel, who pulled it from the cerebral venous blood of rabbits whose brains had been induced into deep sleep by electrical stimulation.
What sets DSIP apart from every other sleep compound: it doesn't sedate. Sedatives — benzodiazepines, Z-drugs, antihistamines — knock you out by depressing the central nervous system. DSIP appears to shift sleep architecture instead, increasing the slow-wave delta activity that defines the deepest, most restorative stage of sleep. You're not pharmacologically unconscious. You're sleeping the way the body wants to sleep.
Here's the strange part: nearly 50 years after DSIP was discovered, researchers still haven't found its receptor. They haven't confirmed where in the body it's produced. They haven't fully mapped its mechanism. What they have is decades of behavioral and physiological data showing it does something — sleep modulation, stress response regulation, pain attenuation, opioid withdrawal effects — across multiple species.
The 1992 double-blind trial in 14 chronic insomniacs (PMID 1299794) showed improved delta-wave sleep without REM suppression. Earlier 1984 research from Larbig and colleagues suggested analgesic effects in chronic pain patients. Russian and Eastern European literature has explored DSIP for opioid withdrawal for decades. Over 150 PubMed citations. None of it explains how the peptide actually works at the molecular level. That gap is exactly why DSIP keeps showing up in research labs — and exactly why it's never reached pharmaceutical commercialization.
The mechanism is unsolved. The receptor is unknown. The clinical literature is uneven — promising signals across decades, but no large modern Phase 3 trials. A 2001 editorial in the European Journal of Anesthesiology called DSIP "incredibly safe" because no published research had ever recorded a fatal dose in any animal model. The flip side: the FDA cited limited human safety data when it placed DSIP on Category 2 in 2023.
That changed recently. On April 15, 2026, the FDA removed DSIP (Emideltide) from Category 2 after the original nominations were withdrawn. The Pharmacy Compounding Advisory Committee is scheduled to review DSIP on July 24, 2026, evaluating it for inclusion on the Section 503A Bulk Drug Substances List for opioid withdrawal, chronic insomnia, and narcolepsy. As of May 2026, DSIP sits in regulatory transition — no longer formally restricted, not yet formally approved for compounding. Sales as a research compound continue legally.
Here's what's specific to DSIP: it's a small peptide with a notoriously short biological half-life — about 15 minutes due to a specific aminopeptidase that cleaves it rapidly. That instability means cheap synthesis routes and poor storage produce degraded product before it reaches your bench. Inactive DSIP looks identical on a label. It just doesn't do anything in your assay.
Generic Peptides supplies research-grade DSIP for sale at 99% purity, manufactured in the USA. Domestic synthesis with documented sequence integrity — the part that matters when half-life is measured in minutes.
Order DSIP for sale in the USA — 99% purity, full WAGGDASGE sequence, manufactured domestically.
Yes — DSIP is legally available as a research compound in the United States. As of April 15, 2026, it has been removed from the FDA's Category 2 list, with PCAC review scheduled for July 24, 2026 to determine its compounding status. It's not FDA-approved for human use.
Correct, and it's been almost 50 years. Despite extensive research, the specific receptor DSIP binds to has never been identified. Some research suggests it interacts with the MAPK cascade and may be regulated by glucocorticoids. The mechanism remains genuinely open.
Yes. Emideltide is the official designation the FDA uses in the Federal Register and PCAC documentation. DSIP is the original research name from the 1970s. Same 9-amino-acid peptide either way.
Melatonin signals circadian timing — it tells your body when to sleep. DSIP appears to influence sleep architecture itself, specifically the delta-wave (deep) stages. They operate at completely different levels of sleep regulation, and animal research has used them in combination to study sleep onset versus sleep depth separately.
Probably not at the same purity or stability. DSIP's 15-minute biological half-life means synthesis quality and storage matter unusually much. Cheap product is often degraded before delivery, and you can't tell visually. You find out when your assay produces nothing.
Sources
Schneider-Helmert D, Schoenenberger GA — original DSIP characterization research from the University of Basel/Bern, 1977. Documents the discovery, isolation, and 9-amino-acid sequence. https://pubmed.ncbi.nlm.nih.gov/?term=schoenenberger+DSIP
Schneider-Helmert D, Schoenenberger GA — "Effects of DSIP on chronic insomnia," 1992 double-blind clinical trial. Documents the 14-patient delta-wave sleep improvement without REM suppression. https://pubmed.ncbi.nlm.nih.gov/1299794/
Larbig W et al. — "Therapeutic effects of delta-sleep-inducing peptide (DSIP) in patients with chronic, pronounced pain episodes." European Neurology, 1984. Supports analgesic research applications. https://pubmed.ncbi.nlm.nih.gov/6094192/
FDA — "Bulk Drug Substances Nominated for Use in Compounding Under Section 503A," updated April 22, 2026. Documents Emideltide (DSIP) removal from Category 2 and the July 24, 2026 PCAC consultation. https://www.fda.gov/media/94155/download
A peptide this old, this researched, and this unsolved deserves sourcing that matches. 99% purity, USA-made.
DSIP (Delta Sleep-Inducing Peptide) ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its nonapeptide structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24–36 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~6 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — DSIP contains a tryptophan residue that's particularly prone to photodegradation. | Always keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Signs of Degradation | Healthy powder is white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
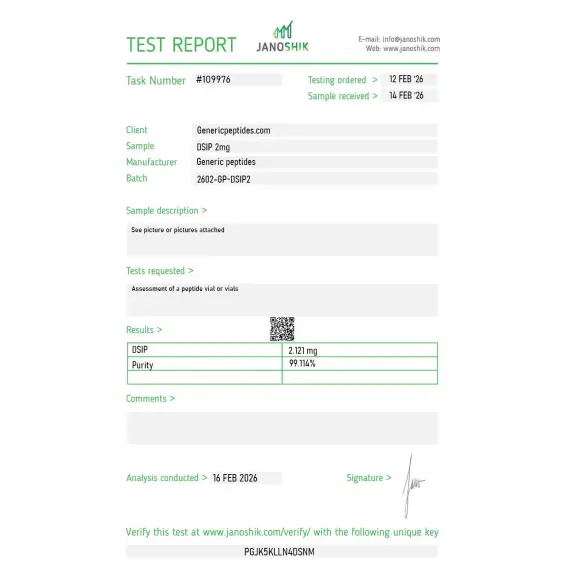
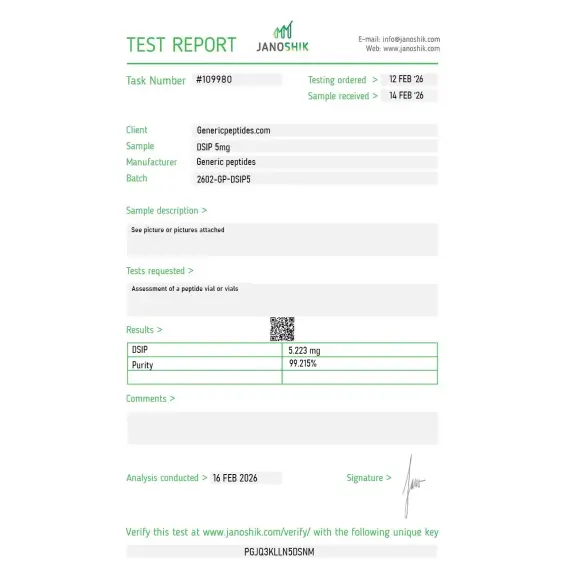
Independent lab test reports are available for DSIP 2mg and 5mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

Schoenenberger and Monnier pulled this out of rabbit cerebral blood in the seventies and the mechanism is still genuinely murky decades later — which is honestly part of why we work on it. The listing doesn't pretend the biology is settled, and that restraint is what I want from a vendor for a compound this poorly understood. Material's been steady in our assays.
Nonapeptide, dissolved without trouble. The reason for four rather than five is that DSIP is reportedly prone to spontaneous changes in solution — there's literature on it cyclizing or degrading depending on conditions — and the documentation said nothing about how to store the reconstituted material. We worked it out conservatively. A handling note specific to this peptide's instability would help.
Reorder. No issues.
We run it next to Selank and Semax as part of a broader look at the older neuropeptide-research tradition — different origins, but a similar pattern of strong early claims and thin modern follow-through. Sourcing them together keeps the comparison clean. DSIP's held up across orders.
The name oversells it, frankly — "delta sleep-inducing peptide" is a 1977 description that the subsequent evidence never really nailed down, and the listing using the historical name without leaning on the sleep claim is the honest way to handle it. We study it for its broader stress-response signaling, not the sleep angle. Behaved as expected.
Reconstituted clean, ran consistently in our binding work. We aliquot single-use and keep it cold given the solution-instability reports — more caution than a typical nonapeptide needs, but it preserves the material. Sequence checked out by mass spec against the synthesis.
Our reference for the delta-sleep-peptide line, such as it is. Repeated orders, consistent. The biology remains a question mark, which is precisely why we keep working with it.
The honest answer is that nobody fully knows. Research suggests DSIP interacts with components of the MAPK signaling cascade and shows homology with glucocorticoid-induced leucine zipper (GILZ). It also appears to stimulate acetyltransferase activity through alpha-1 receptors in rats. The downstream behavioral effect on slow-wave sleep is well-documented; the upstream mechanism is still being mapped.
Most sleep compounds work through GABAergic, melatonergic, or histaminergic systems — well-characterized pathways with known receptors. DSIP doesn't fit any of those categories. It influences sleep architecture without sedation, which makes it mechanistically distinct from nearly every other sleep-related compound in research literature.
Russian and Eastern European literature explored DSIP for stress adaptation and antioxidant effects extensively in the 1990s and 2000s. A 2011 paper by Bondarenko and colleagues described "strong antioxidant effects" through activation of natural defense mechanisms in rats. Animal studies have also shown anticonvulsant and antiedematic effects.
The peptide has a notoriously short biological half-life — around 15 minutes — due to a specific aminopeptidase that cleaves it. That instability means storage conditions and synthesis quality affect bioactivity dramatically. Cheap suppliers often deliver degraded product that looks identical to fresh material on the label.
DSIP was discovered in 1977 by Schoenenberger and Monnier at the University of Basel, working with rabbit brain venous blood during electrically-induced sleep. The peptide has been continuously studied since then, with over 150 PubMed citations spanning sleep, stress, pain, and opioid withdrawal research.
DSIP is not specifically listed by name on the WADA Prohibited List as of 2025. However, athletes subject to drug testing should consult their governing body's specific rules — anti-doping rules can include unspecified substances under broad categories, and individual sport regulations may differ.
Emideltide (the FDA's official designation), Delta Sleep-Inducing Peptide, Delta Sleep Peptide. The amino acid sequence WAGGDASGE identifies it unambiguously regardless of label. The CAS number is 62568-57-4.
Sleep architecture research and stress response biology lead by volume. Pain modulation studies (the 1984 Larbig research) opened a chronic pain research thread. Opioid withdrawal investigations have continued in Russian and European literature. There's also active work in oxidative stress and neuroprotection, particularly in aging-related models.
Short answer: poorly. The native peptide has limited blood-brain barrier penetration, which is part of why some recent research has focused on DSIP fusion peptides combined with cell-penetrating sequences (like Tat) to improve CNS delivery. The 2024 Pichia pastoris fusion peptide research explored exactly this approach.
Melatonin and amino acid precursors (tryptophan, glycine, GABA) work through well-known signaling systems with identified receptors. DSIP appears to operate through an entirely different mechanism — one researchers haven't fully characterized in nearly five decades. That mechanistic gap is part of what keeps it relevant for sleep research even as more conventional compounds dominate clinical use.
Researchers investigating sleep regulation, stress response, and neuropeptide biology often examine DSIP alongside compounds that modulate overlapping neurological and endocrine pathways. Selank is a natural complement — both are short peptides developed for CNS applications with anxiolytic and stress-modulating properties, and researchers studying the relationship between sleep quality and anxiety often examine both simultaneously. Semax targets cognitive function and neuroprotection through ACTH-derived mechanisms, making it relevant in research designs studying the cognitive consequences of sleep disruption and stress. Epitalon shares DSIP's anti-aging research context — both are studied by the Khavinson group and both appear on the July 2026 PCAC review agenda alongside each other, reflecting their overlapping regulatory and research trajectories. MET5 (Met-Enkephalin) modulates endogenous opioid signaling which intersects with sleep architecture and stress response at the neurochemical level. Each represents a different molecular entry point into the same CNS biology that DSIP research addresses.