AICAR 50mg
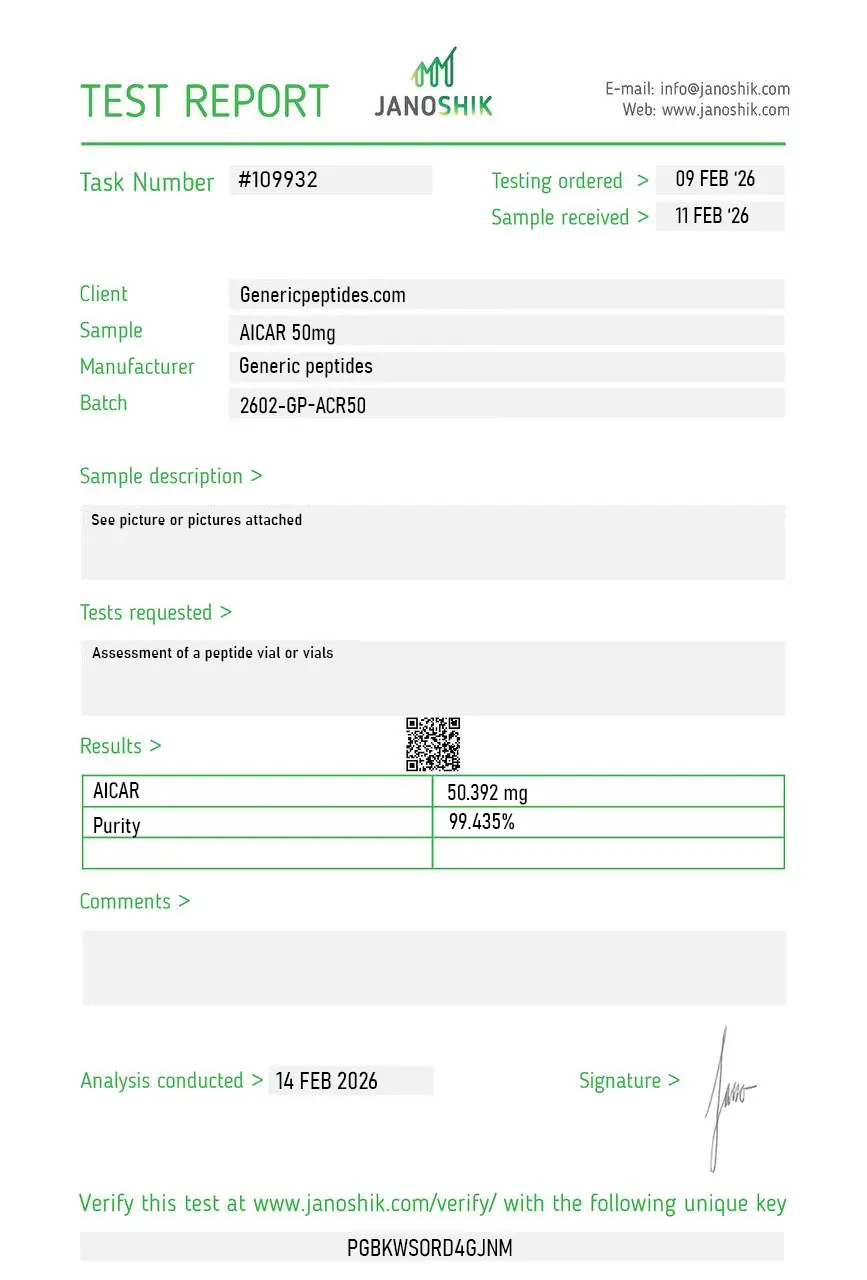
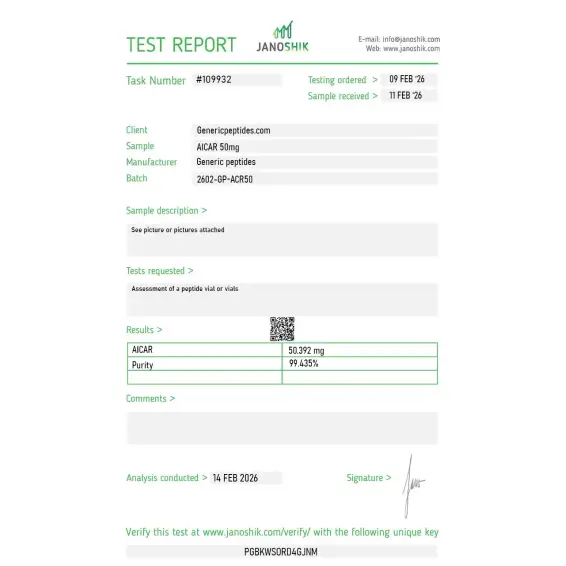
Certificate of Analysis available




Couch-potato mice ran 44% farther than untreated mice after four weeks on a single compound. No training. No diet change. Just AICAR. WADA had it banned within months — before human trials had a chance to finish what the Salk Institute started.
AICAR is a metabolic research compound — not a peptide, despite where it usually shows up in catalogs. It activates AMPK, the enzyme your body relies on as an energy alarm. AMPK normally fires during hard exercise or fasting, telling cells to burn fat and improve fuel efficiency. AICAR triggers it directly. That's why the press called it "exercise in a bottle" in 2008, and why the science world has never quite stopped paying attention.
Ronald Evans and his team at the Salk Institute published their findings in Cell, one of the toughest journals in biology to get into. Sedentary mice treated with AICAR ran 44% longer than untreated controls — no exercise, no training. Evans described it as making muscle "think it's burning fat." WADA added AICAR to the prohibited list in 2009 under Hormone and Metabolic Modulators. Anti-doping agencies don't ban compounds that don't worry them.
The 44% endurance number is real and peer-reviewed. The animal data is some of the strongest in this entire compound category. What nobody should sell you on is a clean human equivalent — that data, at the scale of the Salk study, doesn't exist yet. Anyone guaranteeing you specific human results is making it up.
What's honest to say: AICAR has a deeper research trail than almost anything else in fat-metabolism and endurance biology. Over 1,700 published studies. Phase 3 clinical investigation. That's not a fad — that's a foundation that most compounds in this market couldn't dream of building.
Here's the part most suppliers won't tell you: AICAR is expensive to synthesize at real research-grade purity, which creates an obvious incentive to cut corners. Underdosed and impure batches are everywhere online — and most buyers never find out because they don't have the means to test what they received. For a compound where the entire point is measuring precise biological responses, an impure batch doesn't just underperform. It corrupts your results.
Generic Peptides supplies research-grade AICAR for sale at 99% purity, manufactured in the USA. Domestic sourcing, documented quality, and no guessing about what's actually in the vial. That's the direct response to the quality problem this compound has nearly everywhere else.
Order AICAR for sale in the USA — 99% purity, manufactured domestically.
Correct. AICAR is a nucleoside analog — a small synthetic molecule. It's grouped with peptides by most research suppliers because the buyer overlap is huge, but the chemistry isn't close. The accurate label is metabolic research compound or AMPK activator.
Yes — for research purposes, AICAR is legally available in the United States. It's banned in competitive sports under WADA, so any athlete subject to drug testing should think twice. Outside that context, no legal restriction on purchase as a research compound.
Honestly, that question isn't settled. The animal research is rigorous and well-cited. Human trials at the same scale haven't been completed. That gap is exactly why AICAR remains a research compound and not an approved drug — and why anyone selling it as a guaranteed human performance enhancer is lying.
Same molecule. Acadesine is the pharmaceutical name used in clinical contexts; AICAR is what you'll see in research chemistry and performance science. CAS 2627-69-2 in either case.
Probably not at the same purity. AICAR's synthesis cost doesn't disappear; it just gets passed to you in degraded quality instead. The published research on online research-compound sourcing is not flattering.
Sources
Narkar VA et al. — "AMPK and PPARδ Agonists Are Exercise Mimetics." Cell, 2008. The Salk Institute study documenting 44% endurance increase in sedentary mice treated with AICAR. https://pubmed.ncbi.nlm.nih.gov/18674809/
USADA — Official guidance on AICAR and AMPK activators on the WADA Prohibited List. Supports the 2009 ban context and current classification under Hormone and Metabolic Modulators. https://www.usada.org/spirit-of-sport/aicar-and-other-prohibited-amp-activated-protein-kinase-activators/
PubChem — Acadesine compound entry. Supports product identity, CAS number (2627-69-2), molecular formula (C₉H₁₄N₄O₅), and AMPK activator classification. https://pubchem.ncbi.nlm.nih.gov/compound/Acadesine
Bułdak RJ et al. — "AICAr, a Widely Used AMPK Activator with Important AMPK-Independent Effects." PMC review supporting the breadth of AICAR research applications and citation history. https://pmc.ncbi.nlm.nih.gov/articles/PMC8147799/
Over 1,700 published studies don't happen by accident. The research is serious — the sourcing should match.
AICAR (5-aminoimidazole-4-carboxamide ribonucleoside) ships as a lyophilized powder in a sealed glass vial, freeze-dried to remove water and extend shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F); stable up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | A standard household freezer works — just avoid frost-free units with big temperature swings. |
| Light Sensitivity | Yes — prolonged light exposure can degrade the powder over time. | Keep the vial in its original box or a dark, opaque container. |
| Freezing | Allowed and recommended for long-term storage. −20°C is standard; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Signs of Degradation | Healthy powder is white to off-white and loose. Watch for yellowing, clumping, visible moisture, or a sticky/damp appearance. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial on a counter after delivery, storing in a bathroom or kitchen cabinet with humidity swings, or opening the vial cold and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
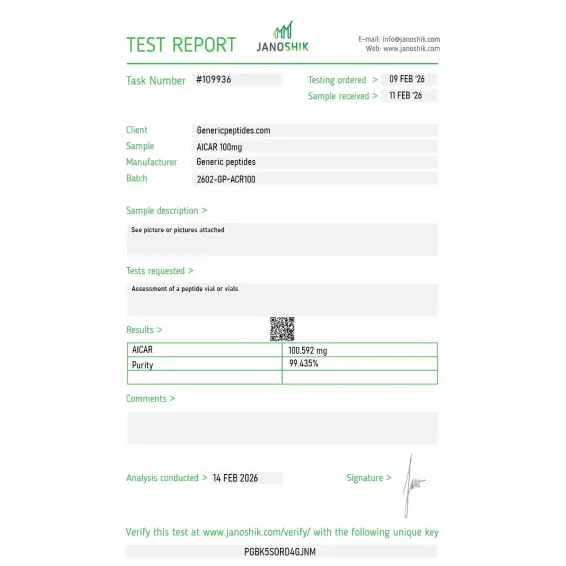
Independent lab test reports are available for AICAR 50mg and 100mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

AMPK activation in our metabolic-signaling work — AICAR phosphorylates to ZMP intracellularly and mimics AMP at the AMPK regulatory site, which is the canonical pharmacological way to switch the pathway on. It's been the standard AMPK probe for decades. Material gave clean pathway activation, consistent with the thousands of papers using it the same way.
The thing I value about AICAR over the trendier metabolic compounds is the depth of literature — this isn't a single-group hypothesis, it's a foundational AMPK probe with decades of independent characterization across countless labs. When a reagent has that much corroboration behind it, batch quality is really the only variable, and this material has held steady.
We use it as the positive control for AMPK activation when screening other candidate activators — it's the reference every metabolic lab benchmarks against, so the comparison only means anything if the AICAR itself is reliable. Across orders it's been consistent enough to trust as the anchor. That's the whole job of a reference standard.
Quality of the product itself has been good across two orders. I'd give five stars if the website search worked better — I had to scroll through the metabolic category to find AICAR because the search returned unrelated results. Minor thing, but worth mentioning.
Dissolved without trouble — it's reasonably water-soluble as the sodium salt, unlike some of the peptides we handle. Standard small-molecule handling, room-temperature stable as the solid, no special freeze-thaw anxiety. Ran consistently in our AMPK-phosphorylation readouts. Refreshingly low-maintenance compared to the labile peptides in our freezer.
Our standard AMPK activator, full stop. Decades of literature behind the molecule, and this supplier's material has been consistent enough across repeated orders that it just does its job as the reference probe. Nothing more I need from it.
Showed up Thursday. Didn't expect it that fast honestly. Box looked like someone actually gave a shit packing it which is more than I can say for a couple other places I've tried. I'll be back.
AICAR enters cells and gets converted into ZMP, a molecule that mimics AMP — the signal cells release when their energy is running low. That false signal flips on AMPK, the same enzyme that activates during real exercise or fasting. The cell responds by burning fat, improving glucose uptake, and shifting toward energy efficiency.
They're often mentioned together because both came out of the same 2008 Salk study, but they hit different targets. Cardarine activates PPARδ — a different metabolic switch — and required exercise to show its strongest effects. AICAR works on AMPK and produced the 44% endurance result in completely sedentary animals.
A lot. AMPK activation pushes cells toward burning fatty acids instead of storing them, which is why AICAR keeps showing up in fat-metabolism research and obesity-related studies. Animal data consistently shows reduced fat accumulation and improved lipid profiles, though human translation hasn't been studied at the same scale
Synthesizing AICAR at 99% purity requires precise chemistry and quality control that costs money. Suppliers who cut corners on synthesis or skip purification steps can sell it cheaper — but the result is contaminated material that distorts research outcomes. Most online buyers have no way to verify what they received.
AICAR has been in scientific literature since the late 1980s, originally explored for cardiac protection and metabolic disease. Its profile changed dramatically after the 2008 Salk Institute paper in Cell, which reframed it as an "exercise mimetic" and triggered the 2009 WADA ban.
Acadesine, AICA riboside, 5-Aminoimidazole-4-carboxamide ribonucleoside, and the brand name Aicaride in some pharmaceutical contexts. CAS number 2627-69-2 identifies the same molecule across all of them. You'll see different names depending on whether the source is clinical, research, or sports science.
It's the textbook example of a direct AMPK activator — most papers studying AMPK use AICAR as the standard tool to turn the pathway on. There are newer AMPK activators in development, but none have AICAR's published track record.
Fat-metabolism and endurance biology lead the list. It also shows up in cardiac ischemia research, oncology studies on cancer cell metabolism, and diabetes-related work on insulin sensitivity. The compound's reach across so many research areas is part of why its citation count keeps climbing.
It wasn't tested as a fat-loss drug — it was investigated under the name acadesine for protecting heart tissue during cardiac surgery and for treating chronic lymphocytic leukemia. Those trials produced mixed results, but they're the reason AICAR has more clinical exposure than most compounds in this category.
Most metabolic compounds work indirectly — they push cells into stress states that activate AMPK as a side effect. AICAR hits AMPK directly through the same site that natural AMP uses, making it the cleanest tool for isolating AMPK's role in any given experiment. That direct activation is exactly what made the Salk study possible.
Researchers investigating metabolic regulation and mitochondrial function often pair AICAR with compounds that activate overlapping or complementary pathways. AOD 9604 and HGH Fragment 176-191 both target fat metabolism through growth hormone-related mechanisms — different molecular entry points than AMPK activation but similar downstream lipolysis research applications. 5-Amino-1MQ inhibits NNMT, an enzyme that depletes NAD+ availability in obese adipose tissue, making it a natural complement to AICAR in studies of cellular energy metabolism. Semaglutide and Tirzepatide represent the GLP-1/GIP receptor agonist approach to metabolic research — appetite and insulin-pathway driven rather than AMPK-driven, but researchers studying obesity models often examine both axes. Each targets metabolism through a different molecular entry point; isolating which pathway drives a given phenotype typically requires studying them individually before combining.