AOD-9604 2mg
Certificate of Analysis available




Researchers at Monash University took human growth hormone, sliced off the part responsible for fat burning, and threw away the rest. What they kept was a 16-amino-acid fragment that mobilizes fat without raising blood sugar, IGF-1, or building muscle. They called it AOD 9604 — Anti-Obesity Drug 9604. It made it through six human trials. WADA still bans it.
AOD 9604 is a peptide fragment derived from amino acids 176–191 at the tail end of human growth hormone — with one extra tweak. Researchers added a tyrosine residue at the start of the chain to keep the molecule stable. That stabilized fragment is what carries HGH's fat-burning activity without dragging along the parts that grow muscle, raise IGF-1, or mess with insulin sensitivity. Think of it as HGH with everything except the fat-loss feature switched off.
Metabolic Pharmaceuticals out of Australia developed AOD 9604 as a real obesity drug — not a research curiosity. They ran six human clinical trials with around 900 participants total. The 12-week Phase 2a trial showed treated patients losing 2.6 kg compared to 0.8 kg on placebo. That's modest, but real, and the safety profile across all six trials was clean — no serious adverse events tied to the compound itself.
Then came the 24-week Phase 2b trial in 536 obese patients. The weight loss didn't reach statistical significance versus placebo. Development was terminated in 2007. Here's what's strange: the higher doses worked worse than the lower ones — which the FDA and researchers still don't fully understand. The compound had survived more human safety testing than 95% of research peptides ever get, then walked away from the finish line.
The animal data on AOD 9604 was strong. The early human signal was real. The Phase 2b failure in 2007 is the inconvenient part most vendors don't mention — and you should know it before you order. Anyone selling this as a guaranteed fat-loss compound is rewriting history. WADA also lists it as a prohibited substance under S2 (Peptide Hormones, Growth Factors, and Related Substances) for athletes subject to drug testing.
What's still interesting: AOD 9604 has a safety record few research compounds can match — six clinical trials, ~900 participants, no serious adverse events tied to the compound. It hits fat metabolism through a different angle than GLP-1s like Semaglutide, which is why researchers studying lipolysis pathways and fat-metabolism biology still keep it on the bench. The story isn't over. It's just complicated.
AOD 9604 is a 16-amino-acid sequence with a non-standard N-terminal modification — that tyrosine addition is what makes it AOD 9604 and not just regular HGH Fragment 176-191. Cheap synthesis routes routinely skip the tyrosine, sell the unmodified fragment under the AOD label, and most buyers never know. The FDA has flagged peptide impurities and inconsistent purity as specific concerns with AOD 9604 supply. If you're studying the modified compound, the modification needs to actually be there.
Generic Peptides supplies research-grade AOD 9604 for sale at 99% purity, manufactured in the USA. Domestic synthesis with the correct sequence — including the N-terminal tyrosine that distinguishes this fragment from cheaper substitutes.
Order AOD 9604 for sale in the USA — 99% purity, full sequence with N-terminal tyrosine.
Almost, but not quite. They share the same core sequence from amino acids 176-191 of HGH, but AOD 9604 adds a tyrosine residue at the N-terminus for stability. That single modification gives it longer half-life and stronger lipolytic activity per dose than the unmodified fragment. Many suppliers label them interchangeably; chemically, they aren't.
Yes — AOD 9604 is legally available in the United States as a research compound. It is not FDA-approved for human use, and in December 2024 the FDA proposed excluding it from the 503A bulk drug substances list for compounding. WADA prohibits it for athletes in competition. Outside those contexts, it remains a research compound.
Honestly, it means the question is unsettled. Earlier trials showed modest fat loss; the larger Phase 2b didn't reach statistical significance, and oddly, higher doses worked worse than lower ones. Researchers still debate whether the failure was about the dose, the formulation, or species differences from the animal models.
No — and that's the entire point of the design. The 176-191 fragment was specifically chosen to isolate the lipolytic activity of HGH while leaving out the parts that drive IGF-1 release or affect insulin sensitivity. Multiple clinical trials confirmed this separation in humans.
Probably not the same. Without the N-terminal tyrosine modification, you're getting unmodified Fragment 176-191, which has shorter half-life and weaker activity per dose than true AOD 9604. The price gap reflects synthesis complexity, not pure markup.
Sources
Heffernan M, Summers RJ, Thorburn A et al. — "The effects of human GH and its lipolytic fragment (AOD9604) on lipid metabolism." Endocrinology, 2001. Foundational research on AOD 9604's lipolytic mechanism. https://pubmed.ncbi.nlm.nih.gov/11564668/
Stier H, Vos E, Kenley D — "Safety and Tolerability of the Hexadecapeptide AOD9604 in Humans." Journal of Endocrinology and Metabolism, 2013. Reviews the safety record across six clinical trials and ~900 participants. https://www.jofem.org/index.php/jofem/article/view/213/278
FDA Bulk Drug Substance Nomination Document — Documents the 12-week 2.6 kg vs 0.8 kg trial result, the 2007 termination after the Phase 2b failure, and the 2024 FDA decision on the 503A list. https://downloads.regulations.gov/FDA-2024-N-4777-0002/attachment_4.pdf
Cox HD et al. — "Detection and in vitro metabolism of AOD9604." Drug Testing and Analysis, 2015. Supports WADA prohibited-status context and analytical detection methods. https://pubmed.ncbi.nlm.nih.gov/25208511/
A 16-amino-acid fragment with one critical modification. Get the right sequence — or you're not actually researching AOD 9604.
AOD 9604 ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve the peptide's structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — protect from direct light and UV exposure to prevent photodegradation. | Keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | AOD 9604 contains two cysteine residues, which are prone to oxidation if the vial seal is compromised or the powder is exposed to air. | Keep the aluminum crimp cap intact and don't open the vial until ready to reconstitute. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
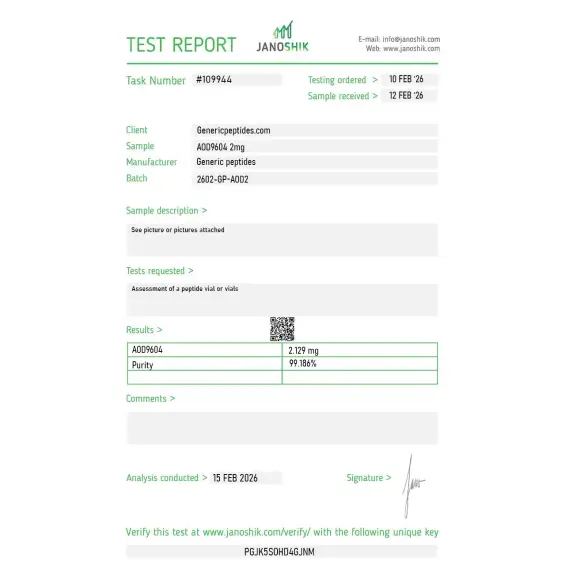
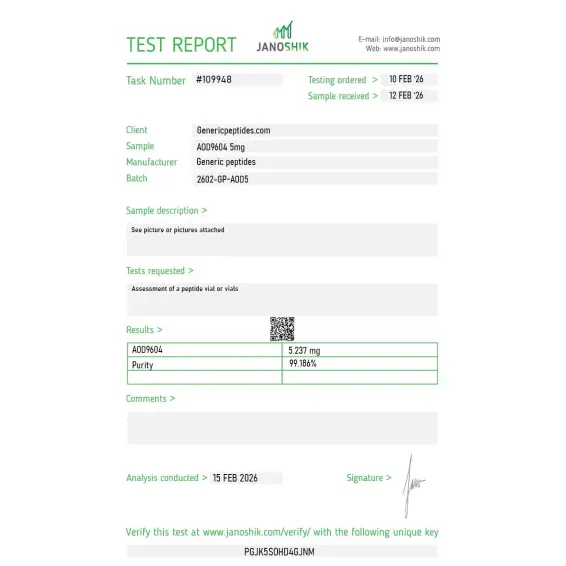
Independent lab test reports are available for AOD-9604 2mg and 5mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

Reorder. Dissolved clean.
We run AOD against the bare HGH Fragment 176-191 to characterize what the tyrosine modification actually buys you in stability and receptor interaction — modified versus unmodified parent. Both from one catalog, matched documentation, clean comparison. AOD held its profile across the conditions.o.
The Metabolic Pharmaceuticals and Monash lineage is the real story — this came out of Frank Ng's fragment work and an Australian biotech's attempt to develop a lipolytic that wouldn't touch the GH-receptor or IGF-1 axis. That functional separation is genuinely interesting pharmacology even though the clinic didn't pan out. Material's been steady.
Reconstituted clean, ran consistently in our lipolysis-pathway assays. We aliquot single-use as standard. The functional dissociation — lipolytic signaling without the IGF-1 stimulation full hGH produces — is precisely why it's a useful probe for isolating that pathway, and the material delivered that cleanly.
Our modified-fragment reference for the lipolysis line. Repeated orders, consistent. The compound's clinical story ended in a failed trial, which is exactly the kind of thing the popular framing leaves out — but as a defined research tool it does what we need.
Niche compound handled professionally. AOD isn't a peptide that every supplier carries with proper documentation, so I appreciated being able to order it here with a COA that referenced the specific batch rather than a generic certificate. Pricing is reasonable for the purity grade. Vial integrity and labeling have been consistent across two orders.
3rd order. At this point it's just automatic — I know what I'm getting and when it'll show up. No drama, no chasing tracking numbers, no excuses. Just a place that works.
AOD 9604 stimulates lipolysis — the breakdown of stored fat — while suppressing lipogenesis, the process that creates new fat deposits. It does this through receptor pathways that researchers believe involve β3-adrenergic receptors, separate from the classical HGH receptor route. That's why it doesn't raise IGF-1 or affect blood sugar.
Different mechanisms entirely. GLP-1s work on appetite signaling — you eat less and feel full longer. AOD 9604 works directly on fat-cell metabolism, telling cells to release stored fat for energy. One controls how much you eat; the other targets how the body handles fat that's already there.
No — that's the deliberate design. The 176-191 fragment was selected specifically because it isolates HGH's fat-metabolism activity without the somatogenic (growth-promoting) effects on muscle, bone, or other tissues. Researchers studying body composition use it specifically when they want to study fat without confounding muscle changes.
The compound's defining feature is the tyrosine residue added to the N-terminus — and adding it correctly during synthesis takes proper solid-phase peptide chemistry. Suppliers cutting corners produce unmodified Fragment 176-191 or sequences with peptide impurities, then sell them under the AOD label. The FDA has flagged this exact issue.
A surprising secondary research thread. Animal studies suggested AOD 9604 may influence cartilage metabolism in osteoarthritis models, which is why some research groups continued working with it after the obesity drug program ended. The evidence is preliminary but distinct from its fat-metabolism profile.
The compound was developed at Monash University in Australia during the 1990s and licensed to Metabolic Pharmaceuticals. Clinical development ran from roughly 2001 through 2007, when the Phase 2b trial led to program termination. The patent and research record date back nearly three decades.
Yes. WADA classifies AOD 9604 as a prohibited substance under category S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). It's banned in and out of competition. Athletes subject to drug testing under WADA-affiliated organizations should avoid it.
You'll see it called AOD-9604, AOD9604, Anti-Obesity Drug 9604, and (loosely) HGH Fragment 176-191 — though the latter technically refers to the unmodified version without the N-terminal tyrosine. The CAS number is 221231-10-3 for the modified compound.
After the obesity program ended in 2007, the licensing rights changed hands and a partner explored cosmetic applications based on the lipolytic activity. The pivot reflected commercial reality more than science — the safety record meant the compound could move into less-regulated markets even after pharmaceutical development stopped.
Tesofensine works centrally — it modifies neurotransmitters that control appetite and energy expenditure. AOD 9604 works peripherally on fat cells themselves, with no significant CNS activity. The difference matters for researchers trying to isolate peripheral fat metabolism from central appetite regulation in study design.
Researchers studying growth hormone-derived fat metabolism often examine AOD 9604 alongside compounds that target adipose tissue through related or complementary pathways. HGH Fragment 176-191 shares the same GH C-terminal origin — the two peptides are structurally related and often compared directly in lipolysis research to isolate which sequence modifications drive specific effects. Semaglutide and Tirzepatide represent the GLP-1/GIP receptor approach to fat loss — hormonally driven appetite and insulin signaling rather than direct lipolytic activity, but with the most extensive human clinical dataset currently available for comparison. AICAR activates AMPK and affects fat oxidation through cellular energy sensing, providing a mechanistically distinct tool for studying the same metabolic outcomes. Adipotide targets the vasculature of white adipose tissue directly — a completely different mechanism that researchers sometimes examine alongside AOD 9604 when studying targeted vs systemic approaches to fat reduction.