GHRP-6 5mg
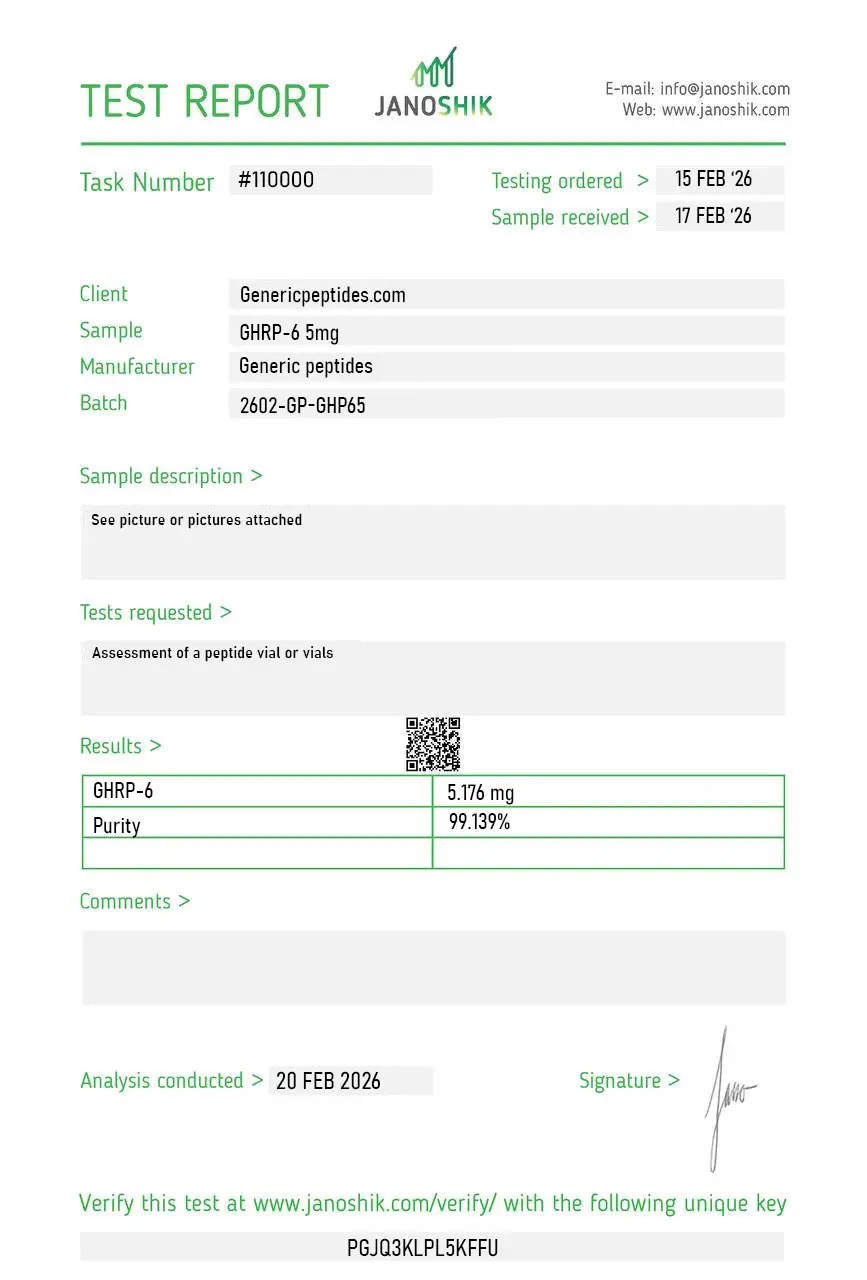
Certificate of Analysis available






Cyril Bowers and his team at Tulane University engineered the first ghrelin receptor agonist before ghrelin itself was even discovered. They knew there had to be a separate pathway for growth hormone release — they just didn't know what natural molecule used it. So they built one. That synthetic hexapeptide was GHRP-6, and it's the compound that opened the entire GHS-R research field.
GHRP-6 (Growth Hormone-Releasing Peptide-6) is a synthetic hexapeptide — six amino acids in the sequence His-D-Trp-Ala-Trp-D-Phe-Lys-NH₂. It's the original member of the GHRP family, developed in the late 1970s and early 1980s by Bowers' group as a synthetic agonist of what was then called the "growth hormone secretagogue receptor" — the receptor for which the natural ligand (ghrelin) wouldn't be identified until 1999.
That's an unusual scientific story. Researchers built a drug for a receptor before anyone knew what the receptor was actually for in normal biology. GHRP-6 is what made the GHS-R discovery possible — it was the molecular probe that helped researchers find ghrelin in the first place.
GHRP-6 binds the same receptor (GHS-R1a) that ghrelin uses. When ghrelin was finally identified in 1999 by Kojima and colleagues at the Kobe University Graduate School of Medicine, the entire GHRP-6 research history suddenly became foundational ghrelin research. Every paper using GHRP-6 to map GH secretion, hunger signaling, gastric motility, or cardiac protection was retroactively part of the ghrelin literature.
What also became clear: GHRP-6 stimulates appetite — strongly. Much more strongly than GHRP-2 or Ipamorelin. That hunger effect made it less attractive as a clean GH research tool but more interesting for studying ghrelin's role in feeding behavior, gastrointestinal motility, and metabolic regulation. The compound has stayed in research because it does something the cleaner secretagogues don't: it gives you the full ghrelin response, hunger included.
Here's the part that matters for study design: GHRP-6 is the least selective of the major GHRPs. It produces strong GH release, but with measurable cortisol elevation, prolactin increases, and pronounced appetite stimulation. For pure GH research without confounding hormonal noise, Ipamorelin is the cleaner choice. GHRP-2 sits in the middle. GHRP-6 is the right tool specifically when researchers want the full ghrelin response — including the appetite and gastric effects — not when they're trying to isolate GH biology cleanly.
Regulatory note: GHRP-6 is not on the FDA's approved 503A bulks list and cannot be compounded by 503A pharmacies. The old Category 1/2/3 framework was replaced by January 2025 FDA guidance. GHRP-6 has no current PCAC review scheduled. WADA prohibits GHRP-6 for athletes in tested sports under category S2. As a research compound, it remains commercially available in the United States.
Here's a sourcing problem that hits GHRP-6 specifically: it contains two tryptophan residues at positions 2 and 4 of the hexapeptide sequence, which makes it unusually prone to oxidation during synthesis and storage. That's not a hypothetical problem — oxidized tryptophan residues change receptor binding and can produce wildly inconsistent bioactivity from batch to batch. Cheap synthesis routes and poor storage conditions accelerate the oxidation. By the time you receive the vial, you may have a compound that looks fine on a label but has degraded enough to skew your results.
Generic Peptides supplies research-grade GHRP-6 for sale at 99% purity, manufactured in the USA. Domestic synthesis with oxidation control during production and storage — the part that matters when tryptophan stability defines whether your assay works.
Order GHRP-6 for sale in the USA — 99% purity, oxidation-controlled synthesis, manufactured domestically.
Yes — GHRP-6 is legally available as a research compound in the United States. It is not on the FDA's approved 503A bulks list and cannot be compounded by licensed pharmacies. WADA prohibits it for tested athletes. Sales as a research compound continue legally.
GHRP-6 is the first-generation compound; GHRP-2 was engineered as an improvement. GHRP-2 produces stronger GH release per dose with somewhat cleaner side effect profiles — less prolactin and cortisol activation, less aggressive appetite stimulation. GHRP-6 still has its place in research specifically because the appetite effect is part of what's being studied.
Yes, more than any other GHRP at standard research concentrations. The hunger effect is one of GHRP-6's defining features and the reason it became a tool for studying ghrelin biology rather than a clinical GH drug candidate. If appetite stimulation would confound your study, GHRP-6 is the wrong choice; if it's the variable you're studying, it's the right one.
Probably not at the same purity or stability. GHRP-6's tryptophan residues oxidize easily, and budget synthesis routinely produces partially oxidized product or material that degrades quickly during storage. Cheap GHRP-6 often looks fine on a label but has lost significant bioactivity by the time it reaches your bench.
GHRP-6 was developed before ghrelin was discovered. When ghrelin was identified in 1999 as the natural ligand for the receptor GHRP-6 was already known to activate, GHRP-6 retroactively became one of the foundational tools of ghrelin research. They target the same receptor (GHS-R1a) — GHRP-6 is essentially a synthetic ghrelin mimetic that came first historically.
Sources
Bowers CY, Momany F, Reynolds GA, Hong A — "On the in vitro and in vivo activity of a new synthetic hexapeptide that acts on the pituitary to specifically release growth hormone." Endocrinology, 1984. The foundational research establishing GHRP-6's pharmacology. https://pubmed.ncbi.nlm.nih.gov/6092043/
Kojima M, Hosoda H, Date Y et al. — "Ghrelin is a growth-hormone-releasing acylated peptide from stomach." Nature, 1999. The discovery of ghrelin as the natural ligand for the receptor GHRP-6 was already known to activate. https://pubmed.ncbi.nlm.nih.gov/10604470/
Arvat E et al. — "Endocrine activities of GHRPs in normal subjects." Comparative human pharmacology data on GHRP-6 vs GHRP-2 vs GHRH establishing relative cortisol/prolactin effects. https://pubmed.ncbi.nlm.nih.gov/9174965/
FDA — "Bulk Drug Substances Nominated for Use in Compounding Under Section 503A," updated April 22, 2026. Documents current compounding status of GHRP-6. https://www.fda.gov/media/94155/download
The original ghrelin mimetic. Tryptophan stability is everything. 99% purity, USA-made.
GHRP-6 ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its hexapeptide structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 18–24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — GHRP-6 contains two tryptophan residues that are particularly prone to photodegradation. | Always keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | The two tryptophan residues also make GHRP-6 susceptible to oxidation if the vial seal is broken or the powder is exposed to air. | Keep the aluminum crimp cap intact until ready to reconstitute. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
Independent lab test reports are available for GHRP-6 5mg and 10mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.
Fine. The detail I'd flag is that GHRP-6 and GHRP-2 get shelved next to each other and look identical as lyophilized powder, and a mislabel between them would quietly wreck an appetite-versus-GH experiment because the balance is reversed between the two. Ours was correctly labeled. Just keep them apart.
Strongest orexigenic of the GHRPs, which is the only reason we use it — appetite-circuit work, not the GH side. Did the job.
No issue with the compound itself across two orders. My complaint is that everyone treats GHRP-6 as a GH thing and the appetite biology — which is genuinely the more distinctive part — gets no shelf space in the description. I do feeding-circuit work and have to bring all the context myself.
Three of us in the lab independently ended up ordering GHRP-6 for completely different reasons — I'm on gastric-motility signaling, one colleague on the cachexia-model appetite work, another using it just as the orexigenic comparator against GHRP-2. Same vial served all three lines without anyone complaining about the batch. That's a decent sign for a shared reagent.
Bowers' early work on these at Wayne State is worth reading — GHRP-6 was one of the probes that mapped the ghrelin receptor before ghrelin was even found. People forget these compounds predate the hormone they mimic. Material's been solid for our receptor assays.
Solubility in bac water was unremarkable, dissolved fine, no haze. We aliquot and freeze single-use because we run trace concentrations and didn't want to gamble on repeated thaws. Held activity. Nothing dramatic to report, which is what I want.
We needed the whole GHRP set for a receptor-pharmacology series and this slotted in as the high-appetite, lower-GH-potency end of the spectrum. The dissociation between appetite drive and GH release across the family is exactly what we're mapping, and GHRP-6 anchors one corner of it
Ghrelin-receptor assays, two orders, both consistent. We characterize the gut-motility response rather than anything GH-related — the receptor's expressed in gastric tissue and that's our angle. Behaved as the literature said it would.
GHRP-6 binds the ghrelin receptor (GHS-R1a) on pituitary somatotrophs and hypothalamic neurons, activating Gq-coupled signaling that drives calcium influx and downstream GH release. Critically, it also triggers ghrelin's other major effects — appetite stimulation, gastric motility changes, and modest cortisol and prolactin elevation. That's the full ghrelin signature, not just the GH portion.
Both target the same receptor, but the selectivity profiles are very different. Ipamorelin was specifically engineered to activate GHS-R1a without significant cortisol, prolactin, or appetite effects. GHRP-6 produces all of those effects strongly. For clean GH research, Ipamorelin wins; for full ghrelin biology research, GHRP-6 is the more accurate model.
Yes, modestly. Comparative human studies from the Turin research group documented measurable cortisol and prolactin increases with GHRP-6 administration — more than GHRP-2 produces, considerably more than Ipamorelin. The cortisol effect is real and is one of the reasons GHRP-6 lost ground to cleaner secretagogues for clinical research applications.
The hexapeptide contains a tryptophan-tryptophan dipeptide that's unusually prone to oxidation during synthesis and storage. Budget production routinely delivers material with partial oxidation that degrades bioactivity. Without HPLC verification specifically checking for oxidized tryptophan residues, the difference is invisible to buyers.
GHRP-6 was developed by Cyril Bowers and Frank Momany at Tulane University in the late 1970s and early 1980s. The foundational 1984 Endocrinology paper established its pharmacology. Critically, this preceded the discovery of ghrelin (1999) by 15+ years — GHRP-6 was a drug for a receptor whose natural ligand hadn't been identified yet.
Yes. WADA prohibits GHRP-6 for athletes subject to drug testing under category S2 (Peptide Hormones, Growth Factors, Related Substances). All GHRPs and growth hormone secretagogues are covered under this classification. Athletes in tested sports should avoid it regardless of how it's obtained.
Growth Hormone Releasing Peptide-6, Growth Hormone-Releasing Hexapeptide, and SKF-110679 in some early pharmaceutical literature. CAS number 87616-84-0. The salt form most commonly sold is GHRP-6 acetate. The amino acid sequence His-D-Trp-Ala-Trp-D-Phe-Lys-NH₂ identifies it unambiguously.
Ghrelin biology and feeding behavior research lead by volume. There's also active work in gastric motility studies — GHRP-6 stimulates gastric emptying through ghrelin receptors in the gut. Cardioprotective research has explored GHS-R1a activation in cardiac tissue using GHRP-6 as a model agonist. Pediatric GH deficiency diagnosis was an earlier clinical application.
Ghrelin is a 28-amino-acid peptide that requires a fatty acid modification (octanoylation at serine-3) to be biologically active. GHRP-6 is a synthetic 6-amino-acid hexapeptide with no lipid modification. Despite the structural differences, both bind the same GHS-R1a receptor with similar functional outcomes — they discovered ghrelin partly by working backward from compounds like GHRP-6.
GHRP-6 was the first synthetic ghrelin receptor agonist ever made — the original molecular tool for the GHS-R1a pathway. Every other GHRP and secretagogue traces its lineage back to GHRP-6's structure-activity research. It also produces the strongest ghrelin-mimicking response of the GHRP family, including the appetite and gastric effects that more selective secretagogues like Ipamorelin specifically avoid.
Researchers investigating ghrelin receptor pharmacology and growth hormone secretagogue potency consistently examine GHRP-6 alongside compounds that target the GH axis through overlapping or complementary mechanisms. GHRP-2 is the most direct comparison — both are hexapeptide ghrelin mimetics with similar GH-releasing potency, but GHRP-2 produces less appetite stimulation and fewer off-target effects; researchers studying the relationship between ghrelin receptor activation and appetite signaling specifically often choose GHRP-6 over GHRP-2 precisely because of the stronger feeding circuit activity. Ipamorelin represents the selectivity end of the ghrelin mimetic spectrum — weaker GH pulse than GHRP-6 but with essentially no cortisol, prolactin, or appetite stimulation, making it the reference compound when researchers need to isolate clean GH secretagogue activity. Hexarelin sits at the opposite end — the strongest GH-releasing ghrelin mimetic available, useful as a potency ceiling reference in comparative secretagogue research. Mod GRF (1-29) is the standard GHRH receptor pairing for GHRP-6 in dual-receptor GH release research — combining GHRH and ghrelin receptor activation on the same pituitary somatotrophs produces synergistic GH output that neither compound achieves alone.