Ipamorelin 2mg
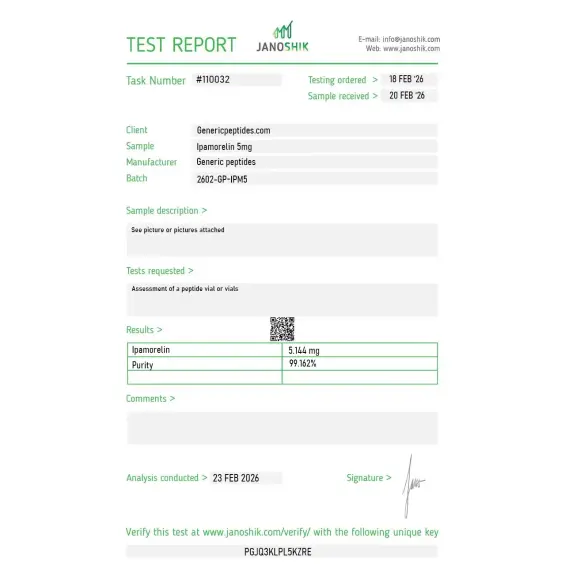
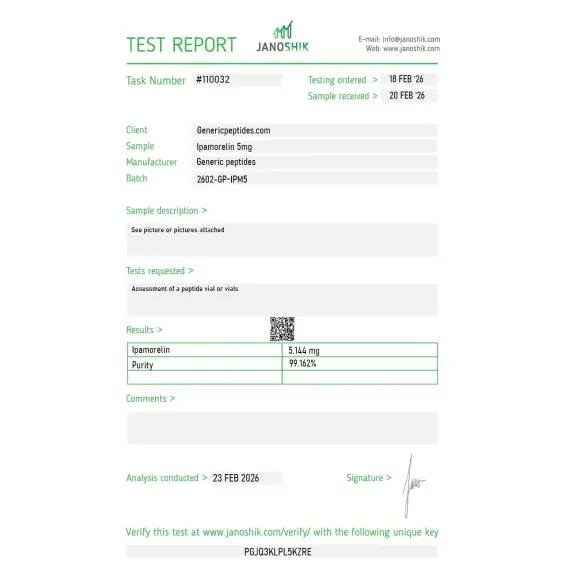
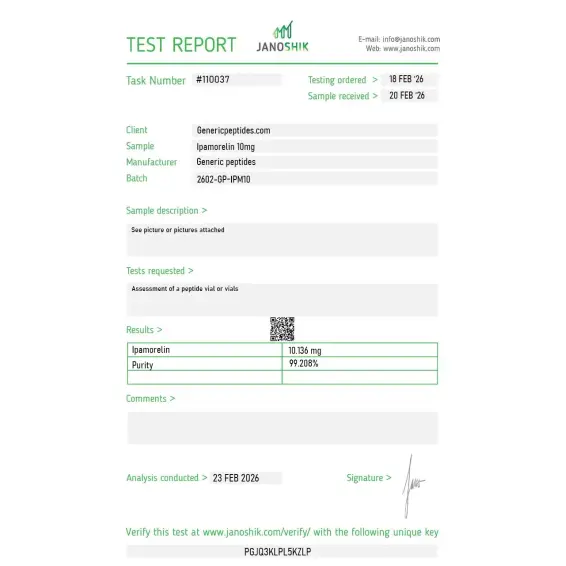
Certificate of Analysis available







Novo Nordisk's research team in 1998 made an explicit design goal: build a growth hormone secretagogue that hits the ghrelin receptor and nothing else. No cortisol elevation. No prolactin. No ACTH. Just GH release. The 1998 Raun paper described what they got: Ipamorelin, the first truly selective growth hormone secretagogue. Even at doses 200 times above the GH-releasing threshold, the off-target hormones stayed flat. That's still the cleanest selectivity profile in the GHRP family.
Ipamorelin is a synthetic pentapeptide — five amino acids: Aib-His-D-2-Nal-D-Phe-Lys-NH₂. It's a selective agonist of the ghrelin receptor (GHS-R1a), the same receptor activated by natural ghrelin and by other GHRPs like GHRP-2 and GHRP-6. What sets Ipamorelin apart isn't the receptor — it's the engineering choices that made it the first truly clean GHS-R1a agonist.
The pentapeptide was developed by Novo Nordisk in the 1990s under the development code NNC-26-0161. It was derived from GHRP-1 with structural modifications specifically chosen to reduce off-target receptor interactions. The result: GH release with minimal effects on cortisol, prolactin, ACTH, FSH, LH, or TSH. Other GHRPs hit one or more of those off-target hormones at clinically relevant doses. Ipamorelin doesn't.
Why does selectivity matter? Because earlier GHRPs muddied every experiment. If you gave GHRP-6 to study GH signaling, you also got cortisol elevation, prolactin spikes, and aggressive appetite stimulation. Untangling which downstream effects came from GH and which came from the off-target hormones became the limiting factor in GHRP research. Ipamorelin solved that problem in one molecule.
The 1998 Raun paper (European Journal of Endocrinology) established the selectivity profile. The 1999 Johansen work demonstrated stimulation of longitudinal bone growth in animal models. The 1999 Oxlund research showed Ipamorelin counteracted glucocorticoid-induced reductions in bone formation — a finding that opened up bone biology research applications independent of GH effects. The 2014 Phase 2 trial for postoperative ileus (Beck et al., International Journal of Colorectal Disease, n=87) is the most rigorous human study published to date.
The honest part Ipamorelin marketing tends to skip: clean selectivity comes with a trade-off — lower absolute GH release compared to less selective GHRPs. Hexarelin produces stronger GH spikes. GHRP-2 produces stronger GH spikes. Ipamorelin's GH response is real but more modest. The trade-off is straightforward: cleaner pharmacology, smaller magnitude. For research designs needing maximum GH stimulation, Hexarelin or GHRP-2 may be the better tools. For research designs requiring isolation of GH-specific effects without confounding hormone responses, Ipamorelin is the only pentapeptide in the family that delivers it.
Regulatory note: Ipamorelin acetate was placed on the FDA's Category 2 bulks list in 2023, then removed from Category 2 in September 2024 after the original nominations were withdrawn. The PCAC reviewed Ipamorelin (acetate and free base) at its October 29, 2024 meeting and voted against adding it to the Category 1 bulks list. As of May 2026, Ipamorelin is not in Category 2, but it's also not in Category 1 — 503A compounding pharmacies cannot legally produce it. WADA prohibits Ipamorelin for athletes in tested sports under category S2.
Here's a sourcing problem that's specific to Ipamorelin: it contains a D-2-Nal residue (D-2-naphthylalanine) — an unusual non-natural amino acid that's expensive and technically demanding to incorporate correctly. Cheap synthesis routes routinely substitute regular naphthylalanine, use the wrong stereoisomer, or fail to incorporate the modified residue at all. The result is a peptide that has the right molecular weight on paper but doesn't bind GHS-R1a with the selectivity that defines real Ipamorelin. Without HPLC-MS verification of the D-2-Nal residue specifically, this defect is invisible to buyers — and it's exactly the difference between Ipamorelin pharmacology and accidentally-running-a-different-experiment pharmacology.
Generic Peptides supplies research-grade Ipamorelin for sale at 99% purity, manufactured in the USA. Domestic synthesis with verified D-2-Nal incorporation — the part that determines whether your selectivity assay produces the literature's profile or noise.
Order Ipamorelin for sale in the USA — 99% purity, D-2-Nal verified, manufactured domestically.
Yes — Ipamorelin is legally available as a research compound in the United States. It was removed from FDA Category 2 in September 2024, but PCAC subsequently voted against Category 1 inclusion at its October 2024 meeting, so it cannot currently be compounded by 503A pharmacies. Sales as a research compound continue legally. WADA prohibits it for tested athletes.
Because it's the only pentapeptide in the family that produces GH release without significantly elevating cortisol, prolactin, ACTH, FSH, LH, or TSH. The 1998 Raun paper documented this selectivity even at doses more than 200-fold above the GH-releasing ED50. Other GHRPs hit at least one off-target hormone at standard research concentrations. Ipamorelin doesn't.
Both target GHS-R1a, but with very different selectivity profiles. GHRP-2 produces stronger absolute GH release but also measurably elevates cortisol and prolactin. Ipamorelin's GH effect is somewhat smaller but cleaner — minimal off-target hormonal activation. Different research tools depending on whether magnitude or selectivity is the experimental priority.
Probably not. The D-2-Nal (D-2-naphthylalanine) residue is the expensive, technically demanding part of Ipamorelin synthesis. Cheap manufacturers routinely substitute regular naphthylalanine, use the wrong stereoisomer, or skip the modification entirely. Without HPLC-MS verification of the modified residue, you may be paying for something that's structurally similar to GHRP-1 mislabeled as Ipamorelin.
Because they target completely different receptors — Ipamorelin hits GHS-R1a, CJC-1295 hits GHRH receptors. Activating both pathways simultaneously produces synergistic GH release roughly 3-5x stronger than either compound alone, while preserving Ipamorelin's selectivity profile. The combination is the most-prescribed GH peptide stack in research and clinical contexts.
Sources
Raun K et al. — "Ipamorelin, the first selective growth hormone secretagogue." European Journal of Endocrinology, 1998. Foundational research establishing Ipamorelin's selectivity profile and pharmacology. https://pubmed.ncbi.nlm.nih.gov/9849822/
Johansen PB et al. — "Ipamorelin, a new growth-hormone-releasing peptide, induces longitudinal bone growth in rats." Documents bone growth research applications. https://pubmed.ncbi.nlm.nih.gov/10373343/
Beck DE et al. — "Ipamorelin in postoperative ileus management." International Journal of Colorectal Disease, 2014. The largest published Phase 2 human trial. https://pubmed.ncbi.nlm.nih.gov/25331030/
FDA — "Bulk Drug Substances Nominated for Use in Compounding Under Section 503A," updated April 22, 2026. Documents Ipamorelin removal from Category 2 (September 2024) and the negative PCAC recommendation. https://www.fda.gov/media/94155/download
The cleanest GHRP only stays clean if the D-2-Nal residue is right. 99% purity, USA-made, modified residue verified.
Ipamorelin ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its pentapeptide structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — protect from direct light and UV exposure to prevent photodegradation. | Keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a frost-free freezer with temperature swings, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
Independent lab test reports are available for Ipamorelin 2mg, 5mg, and 10mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.


Decent for our GH-axis work. The selectivity is real but it depends on synthesis purity — a contaminating related sequence can introduce the cortisol response Ipamorelin is supposed to lack, which would quietly confound an experiment that relies on the clean profile. I'd want tighter impurity documentation for exactly that reason. Material behaved cleanly in our hands, but the risk is why I check.
Ipamorelin's whole value is selectivity — it activates the ghrelin receptor without the cortisol and prolactin spillover that GHRP-2 and GHRP-6 produce. That clean profile is the entire reason it exists as a distinct compound. The vendor frames it that way. Star off because the D-2-naphthylalanine substitution at position 3 — the structural basis for that selectivity — wasn't confirmed on the COA.
GHS-R1a activation in pituitary somatotroph culture. The clean GH-release signal with no measurable cortisol or prolactin response in our parallel measurements is exactly why we use Ipamorelin over the other GHRPs. Consistent.
Raun's 1998 characterization paper out of Novo Nordisk is still the reference for Ipamorelin's selectivity profile, and it's nice the listing points toward the actual literature rather than marketing language. Material gave clean dose-response curves in our receptor work.
What I appreciate about the listing is that it separates Ipamorelin from CJC-1295 mechanistically rather than just selling them as a "stack." They hit entirely different receptors — ghrelin receptor versus GHRH receptor — and lumping them together as marketing does obscures that. Refreshing to see the pharmacology kept straight. Material performed as expected.
The development history is interesting context — Novo took it through clinical trials, then Helsinn licensed it for post-operative ileus, and it never reached approval despite the clean profile. The listing acknowledges that twice-failed clinical path rather than implying it's an established therapeutic. That honesty matters for procurement justification.
For comparative GHRP pharmacology we run all four — GHRP-2, GHRP-6, Hexarelin, Ipamorelin — and Ipamorelin is the clean selective control against the three that produce off-target cortisol and prolactin. Sourcing the whole family from one place keeps the selectivity comparison interpretable. That contrast is the entire experiment.
The selectivity mechanism is genuinely elegant — the naphthylalanine at position 3 is what keeps it from activating the corticotropic pathways the other GHRPs touch. Working with Ipamorelin as the clean reference helps frame what the off-target activity in the dirtier GHRPs actually costs experimentally. Material consistent with that framing.
Ipamorelin binds GHS-R1a (the ghrelin receptor) on pituitary somatotrophs and hypothalamic neurons, activating Gq-coupled signaling that drives calcium influx and GH release. The selectivity is the key feature: at the same receptor binding event, Ipamorelin doesn't engage the secondary signaling cascades that produce cortisol, prolactin, or ACTH effects in less selective GHRPs. The receptor is the same; the downstream pharmacology is cleaner.
GHRP-6 was the first-generation ghrelin receptor agonist with strong GH release but pronounced cortisol, prolactin, and appetite effects. Ipamorelin was specifically engineered for clean GH release without those off-target effects. Trade-off: Ipamorelin's absolute GH release is somewhat smaller than GHRP-6's, but its profile is dramatically cleaner from a hormonal interference standpoint.
At standard research concentrations, yes — published research consistently documents minimal effects on cortisol, prolactin, ACTH, and other pituitary hormones. The 1998 Raun paper tested doses more than 200-fold above the GH-releasing threshold and still found minimal off-target activation. That selectivity is the entire reason Ipamorelin became the preferred GHRP for clean GH research.
The pentapeptide contains a D-2-naphthylalanine (D-2-Nal) residue — an unusual non-natural amino acid that's expensive and technically demanding to incorporate correctly. Cheap synthesis frequently substitutes regular naphthylalanine or uses the wrong stereoisomer, producing material that's structurally similar to GHRP-1 mislabeled as Ipamorelin. Detection requires HPLC-MS specifically targeting the modified residue.
Ipamorelin was developed by Novo Nordisk A/S in the mid-1990s under the development code NNC-26-0161. The foundational characterization paper by Raun and colleagues was published in 1998 in the European Journal of Endocrinology. Bone growth research and postoperative ileus applications followed in subsequent decades, with over 150 PubMed publications by 2026.
Yes. WADA prohibits Ipamorelin for athletes subject to drug testing under category S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). The classification covers all GHRPs. Athletes in tested sports should avoid the compound regardless of how it's obtained.
Ipamorelin acetate (the salt form most commonly sold), NNC-26-0161 (the original Novo Nordisk development code), and the chemical sequence Aib-His-D-2-Nal-D-Phe-Lys-NH₂. CAS number 170851-70-4. Different naming conventions across literature and commercial sources, all referring to the same pentapeptide.
Growth hormone axis pharmacology and selective GHS-R1a research lead by volume. Bone biology research has expanded substantially since the 1999 Johansen and Oxlund papers — particularly studies of glucocorticoid-induced bone loss and longitudinal bone growth. Gastrointestinal motility research (postoperative ileus models) opened a separate research thread that produced the 2014 Phase 2 trial.
Both target GHS-R1a but with opposite design priorities. Hexarelin was engineered for maximum GH release potency, with the trade-off of receptor desensitization, off-target hormonal effects, and CD36 receptor activation. Ipamorelin was engineered for selectivity at GHS-R1a alone, with smaller GH release but minimal off-target effects. Different research tools for different design priorities.
Native ghrelin is a 28-amino-acid peptide requiring octanoylation (a fatty acid modification at serine-3) to be biologically active, and it has multiple receptor effects beyond GH release. Ipamorelin is a synthetic 5-amino-acid pentapeptide that doesn't need lipid modification and is engineered to selectively activate only the GH-releasing aspect of GHS-R1a signaling. Same primary receptor, dramatically simplified pharmacology.
Researchers investigating growth hormone secretagogue pharmacology and pituitary GH axis biology consistently examine Ipamorelin alongside compounds that target the same axis through complementary receptor pathways or contrasting kinetic profiles. Mod GRF (1-29) is the standard pairing — Ipamorelin activates the ghrelin receptor while Mod GRF activates the GHRH receptor on the same pituitary somatotrophs; the matching 30-minute half-lives produce synchronized pulses through both pathways simultaneously, which is why this combination is the most-studied GH peptide stack in the research literature. CJC-1295 DAC replaces Mod GRF when researchers need sustained GH elevation rather than pulsatile release — the same ghrelin receptor activation from Ipamorelin paired with a week-long GHRH receptor signal produces a fundamentally different pharmacokinetic profile for studying chronic GH axis stimulation. GHRP-2 and GHRP-6 are direct ghrelin mimetic comparators — both produce stronger GH pulses than Ipamorelin but with cortisol, prolactin, and appetite off-target activity that Ipamorelin lacks; researchers studying receptor selectivity consequences typically examine all three in parallel. Sermorelin represents the unmodified GHRH sequence reference — useful when researchers need to compare physiological GHRH signaling against engineered ghrelin mimetic activation.