Sermorelin 2mg
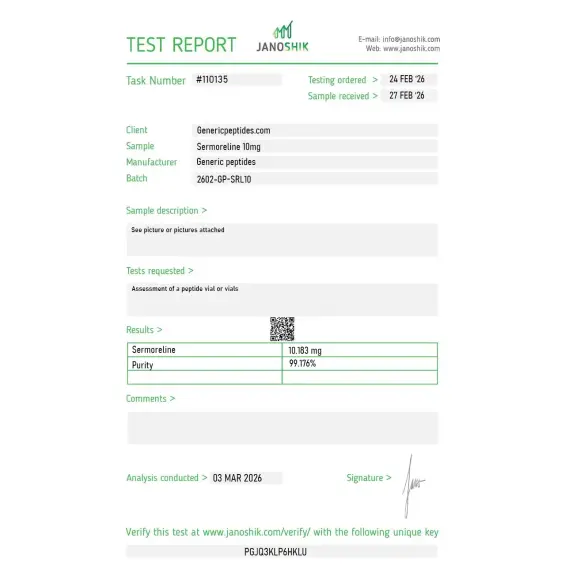
Certificate of Analysis available









Most of the GHRH peptides researchers discuss today are technically experimental compounds that never reached pharmaceutical approval. Sermorelin is the exception. The FDA actually approved it in 1997 under the brand name Geref, both as a diagnostic tool for growth hormone deficiency and as a treatment for children with growth failure. Serono manufactured it commercially for over a decade. Then in 2008, they discontinued production — not because it didn't work, but because the company couldn't make money on it. That voluntary withdrawal is why Sermorelin still exists in regulatory categories that newer GHRH analogs can't reach.
Sermorelin is a synthetic 29-amino-acid peptide identical to the first 29 residues of natural human GHRH (growth hormone-releasing hormone). The naturally occurring GHRH in your body is a 44-amino-acid molecule, but researchers in the 1970s discovered something useful: the entire biological activity lives in the first 29 residues. Cut off the last 15 amino acids and you still have a fully functional GHRH analog. That truncated version is Sermorelin — also called GRF 1-29 NH₂.
The chemistry is what makes Sermorelin pharmacologically distinct from compounds like CJC-1295. Sermorelin is the active GHRH sequence, unmodified. CJC-1295 is the same 29-amino-acid backbone with four amino acid substitutions to resist enzymatic degradation. CJC-1295 with DAC adds an albumin-binding tag for week-long half-life. Sermorelin has none of those modifications — it's structurally identical to natural GHRH, with all the natural pharmacokinetics. Half-life of about 10-12 minutes. Pulsatile signaling. Standard GHRH receptor pharmacology.
This is the part that matters for serious researchers: Sermorelin is a component of a previously FDA-approved drug (Geref, NDA 020443). Under Section 503A of the Food, Drug, and Cosmetic Act, that status makes Sermorelin eligible for compounding pharmacy production — specifically because it meets one of the three statutory criteria for 503A compounding (being a component of an FDA-approved drug). This is the same legal pathway that allows compounding pharmacies to produce certain other formerly-approved drugs that have been discontinued from commercial production.
That puts Sermorelin in a fundamentally different regulatory position from BPC-157, CJC-1295, Ipamorelin, Epitalon, and the other research peptides currently in regulatory transition. Those compounds have never been components of FDA-approved drugs. Sermorelin has. Compounding pharmacies legally produce it under 503A; the others can't be compounded under standard rules. The Frier Levitt regulatory analysis (January 2026) specifically names Sermorelin alongside NAD+ as examples of peptides that legitimately meet 503A compounding criteria. As a research compound, Sermorelin remains commercially available alongside its compounding pathway.
Here's the honest part: Sermorelin's 10-12 minute half-life is a real research limitation. The compound stimulates pulsatile GH release like natural GHRH does, but those pulses are brief. Researchers who need sustained pharmacological GH stimulation typically choose modified analogs (Mod GRF 1-29 or CJC-1295 DAC) instead. Sermorelin is the right tool when natural GHRH-like pulse patterns are the experimental goal — diagnostic GH stimulation tests, physiological pituitary research, comparative pharmacology with synthetic analogs. It's the wrong tool when chronic exposure or amplified signaling is what you need.
Sermorelin also doesn't produce the off-target hormonal effects that earlier GHRPs cause. It's selective for the GHRH receptor (GHRH-R), so cortisol, prolactin, and ACTH stay essentially unchanged at standard research concentrations. That selectivity is what made it useful as a diagnostic tool — clinicians could test pituitary GH reserve without confounding hormonal noise.
Regulatory note: Sermorelin is currently the only GHRH analog with FDA-approved drug status (as Geref, voluntarily withdrawn from commercial production in 2008 for non-safety reasons). It's not on the FDA's Category 2 list — it doesn't need to be, because its FDA-approved drug component status provides a separate compounding pathway. WADA prohibits Sermorelin for athletes in tested sports under category S2 (Peptide Hormones, Growth Factors, Related Substances). Sales as a research compound continue legally alongside the 503A compounding pathway.
Here's a sourcing problem that's specific to Sermorelin: it's the unmodified natural GHRH sequence, which means the four CJC-1295 substitutions that resist enzymatic cleavage aren't present here. That makes Sermorelin particularly vulnerable to handling and storage issues — improper temperature exposure, repeated freeze-thaw cycles, and slow synthesis routes can produce material with significant degradation before it reaches your bench. Cheap producers also routinely confuse Sermorelin with Mod GRF 1-29 (the modified version) and sell one labeled as the other. The two compounds look similar on basic analytical methods but have completely different stability profiles. If you're studying physiological GHRH pulsatility specifically, accidentally getting the modified version means your experiment isn't what you think it is.
Generic Peptides supplies research-grade Sermorelin for sale at 99% purity, manufactured in the USA. Domestic synthesis with the unmodified GRF 1-29 sequence verified — the part that determines whether you have natural GHRH pharmacokinetics or accidentally-purchased-modified-analog pharmacokinetics.
Order Sermorelin for sale in the USA — 99% purity, unmodified GRF 1-29 sequence verified, manufactured domestically.
Yes — Sermorelin is legally available both as a research compound and through compounding pharmacy production. Unlike most GHRH-related peptides currently in regulatory transition, Sermorelin is a component of an FDA-approved drug (Geref, NDA 020443), which makes it eligible for compounding under Section 503A. WADA prohibits it for tested athletes.
Same 29-amino-acid GHRH backbone, but CJC-1295 has four amino acid substitutions that resist enzymatic degradation and extend half-life. Sermorelin's half-life is 10-12 minutes; CJC-1295 (no DAC) is about 30 minutes; CJC-1295 with DAC is 6-8 days. Sermorelin is the unmodified natural sequence; CJC-1295 is the engineered stabilization version.
Commercial reasons, not safety. Serono (the manufacturer) voluntarily withdrew Geref from the US market — the FDA confirmed in a 2013 Federal Register notice that the discontinuation wasn't due to safety or effectiveness concerns. The economics of producing a niche pediatric GH-deficiency drug after recombinant HGH became dominant didn't justify continued manufacturing. The FDA approval status remains intact even though commercial production stopped.
Different pharmacological approach. Recombinant HGH directly supplies growth hormone, often at supraphysiological levels with sustained suppression of natural pituitary signaling. Sermorelin stimulates the pituitary to release its own GH, preserving natural pulsatile patterns and negative feedback regulation. Different research tools depending on whether physiological GHRH-driven biology or pharmacological GH excess is the experimental target.
Probably not at the same purity, and possibly not even the same compound. Cheap suppliers routinely confuse Sermorelin with Mod GRF 1-29 (the modified version with four amino acid substitutions) and sell them interchangeably. They have completely different stability profiles, half-lives, and research applications. Without HPLC-MS verification specifically distinguishing the unmodified sequence from modified analogs, you may be buying something other than what's on the label.
Sources
Prakash A, Goa KL — "Sermorelin: a review of its use in the diagnosis and treatment of children with idiopathic growth hormone deficiency." BioDrugs, 1999. Comprehensive review of clinical efficacy and pharmacology supporting FDA approval. https://pubmed.ncbi.nlm.nih.gov/18031173/
FDA — Federal Register notice on Geref Diagnostic determination, March 4, 2013. Documents the voluntary discontinuation as not due to safety or effectiveness concerns. https://www.federalregister.gov/documents/2013/03/04/2013-04827/determination-that-geref-sermorelin-acetate-injection-05-milligrams-basevial-and-10-milligrams
Frier Levitt — "Regulatory Status of Peptide Compounding in 2025." Documents Sermorelin's eligibility for 503A compounding as a component of an FDA-approved drug. https://www.frierlevitt.com/articles/regulatory-status-of-peptide-compounding-in-2025/
FDA — "Bulk Drug Substances Nominated for Use in Compounding Under Section 503A," updated April 22, 2026. Documents the regulatory framework for GHRH analogs and FDA-approved drug components. https://www.fda.gov/media/94155/download
The original GHRH analog. FDA-approved status. Unmodified sequence integrity matters.
Sermorelin ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its 29-amino-acid GHRH structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — protect from direct light and UV exposure to prevent photodegradation. | Keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | Sermorelin contains a methionine residue that's prone to oxidation if the vial seal is broken or the powder is exposed to air. | Keep the aluminum crimp cap intact until ready to reconstitute. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
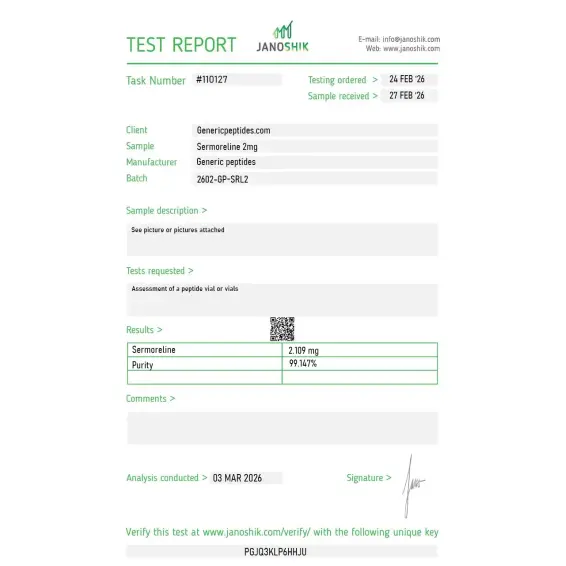
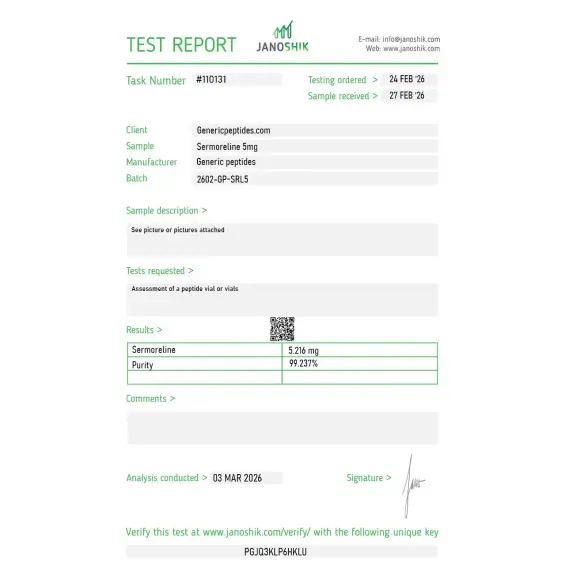
Independent lab test reports are available for Sermorelin 2mg, 5mg, and 10mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.


Native GRF(1-29), our physiologic GHRH reference. cAMP response in somatotrophs as expected.
The reason to pick sermorelin over the modified analogs is precisely that it isn't modified — it's the native human GHRH(1-29) sequence, the physiologic baseline against which you measure what the substitutions in mod-GRF or the DAC version actually do. The vendor distinguishes it from those analogs, which matters. Star off because the COA should confirm the native unmodified sequence, since several analogs share a similar molecular weight.
Guillemin won the Nobel for the hypothalamic hormone work that includes GHRH, and sermorelin is essentially the active fragment of that. Hard to argue with that pedigree as a reference compound. Material gave consistent receptor activation in our pituitary cell work.
Useful precisely because of its short half-life — the DPP-IV cleavage at position 2 means it clears fast, which makes it the right tool when you want acute pulsatile receptor activation rather than the sustained signal you'd get from the DAC analog. Different experimental questions need different kinetics, and this is the pulsatile end of the spectrum.
Reorder. Pituitary somatotroph work. Native sequence, consistent.
What I needed was the diagnostic-grade physiologic reference, the same molecule used in the sermorelin-arginine GH stimulation test, for an in-vitro characterization. The native sequence is the point — modified analogs don't replicate the actual endogenous GHRH signaling profile. Material matched our expectations.
Native GHRH reference, reliable, three orders.
Native GHRH(1-29) reference for our analog panel. Consistent, reordered, nothing more to add.
Wife ordered something from a different company same week I ordered from here. Hers arrived damaged, mine arrived perfect. She now understands why I order from where I order from.
Sermorelin is a synthetic peptide made from the first 29 amino acids of your body's natural growth hormone-releasing hormone (GHRH) — the active portion that actually stimulates growth hormone release. It was originally developed in the 1970s and was FDA-approved (under the brand name Geref) for diagnosing and treating growth hormone deficiency in children. Although the original branded version was discontinued in 2008, Sermorelin is still widely available in the US through compounding pharmacies and is legally prescribed off-label for adult anti-aging, wellness, and hormone optimization clinics.
Sermorelin binds to GHRH receptors on the pituitary gland, signaling the gland to release a natural pulse of growth hormone (GH). The released GH then travels to the liver, where it stimulates the production of IGF-1, which drives muscle growth, fat metabolism, tissue repair, and cellular regeneration. A key feature is that Sermorelin preserves the body's natural negative feedback loop — if GH levels get too high, the system self-regulates. This is fundamentally different from injecting synthetic HGH, which bypasses these regulatory checks entirely.
Most commonly reported benefits include better sleep quality (especially deeper slow-wave sleep), increased lean muscle mass, reduced body fat (particularly abdominal fat), faster recovery from exercise and injury, improved skin elasticity, and increased energy levels. Many users also report improved mood, libido, and cognitive focus. Results tend to be gradual — benefits emerge over weeks to months rather than days. Clinical evidence is strongest for treating GH-deficient children; adult wellness benefits come largely from clinical observation rather than large randomized trials.
Common adult protocols use 200 to 500 mcg injected subcutaneously once daily before bedtime, though doses up to 1,000 mcg are sometimes used. Evening timing is important because it aligns with the natural overnight GH peak, which occurs during deep sleep. Treatment cycles typically run 3 to 6 months with periodic reassessment of IGF-1 blood levels. Starting doses are often on the lower end and titrated up based on response and tolerance. Your specific dose should always be set by a qualified clinician — not copied from online sources.
Most users notice improvements in sleep quality within the first 1–2 weeks, which is often the earliest sign the peptide is working. Better energy levels and recovery typically emerge by weeks 3–6. Visible changes in body composition — increased lean muscle and reduced body fat — generally develop over 3 to 6 months of consistent nightly use combined with appropriate diet and exercise. Older adults with lower baseline GH levels often notice effects more dramatically than younger users with already-healthy hormone levels.
Sermorelin is generally very well tolerated, and side effects are usually mild. The most commonly reported are brief flushing or warmth after injection, mild injection-site reactions (redness, itching, pain), occasional headache, dizziness, nausea, and temporary fatigue. Some users report vivid dreams or mild numbness in the hands. Serious side effects are rare, but Sermorelin can cause water retention and joint discomfort at higher doses, and should not be used by people with active cancer due to its growth-promoting effects on cells.
Most clinicians consider Sermorelin safer than direct HGH injections, for several reasons. Sermorelin works with the body's natural feedback system — your pituitary won't release dangerously high GH amounts because of built-in regulation. Synthetic HGH bypasses these controls entirely and can produce supraphysiological levels that cause insulin resistance, water retention, carpal tunnel syndrome, and other serious side effects. Sermorelin also preserves natural GH production rather than suppressing it. The tradeoff is that Sermorelin produces more modest results than HGH, since it can only stimulate what your pituitary is still capable of releasing.
Yes, Sermorelin is legal in the US when prescribed by a licensed physician and obtained through a legitimate compounding pharmacy under 503A/503B FDA regulations. It is not sold in regular retail pharmacies because its original branded version was discontinued. It is not approved as a finished drug product in most European countries, and research-grade Sermorelin sold online as "not for human consumption" exists in a legal grey area. Athletes should note that Sermorelin is banned by WADA and most sports organizations — competitive athletes using it risk failed drug tests.
Sermorelin is contraindicated for anyone with active cancer or a history of cancer, because GH and IGF-1 can potentially accelerate tumor growth. It should not be used by people with severe obesity (where it may be less effective), uncontrolled diabetes, or active severe illness. Pregnant and breastfeeding women should avoid it, as should children outside of a proper pediatric endocrinology context. People with thyroid disorders, pituitary tumors, or a history of intracranial hypertension should have these conditions fully evaluated and controlled before starting Sermorelin.
All three are growth hormone peptides, but they work through different pathways. Sermorelin and CJC-1295 (Mod GRF) are both GHRH analogs — they stimulate the pituitary via GHRH receptors. Ipamorelin is a ghrelin mimetic that works through a completely different receptor (GHS-R). Sermorelin has a relatively short half-life (~10–20 minutes), similar to Mod GRF. CJC-1295 with DAC lasts much longer (6–8 days). Ipamorelin is often stacked with Sermorelin or CJC-1295 because combining the two pathways produces a stronger, more synergistic GH pulse than either alone — this is why "Sermorelin/Ipamorelin" and "CJC/Ipamorelin" are among the most popular peptide combinations in anti-aging clinics.
Researchers investigating GHRH receptor pharmacology and physiological growth hormone release consistently examine Sermorelin alongside compounds that target the GH axis through complementary receptor pathways or contrasting stability and kinetic profiles. Mod GRF (1-29) is the most direct structural comparison — Mod GRF is the same GRF 1-29 sequence with four amino acid substitutions that extend half-life from ~10 minutes to ~30 minutes; researchers studying the pharmacological contribution of those stability modifications examine both compounds in parallel to isolate sequence engineering effects on GHRH receptor pharmacokinetics. Ipamorelin is the standard ghrelin receptor pairing — combining Sermorelin's GHRH receptor activation with Ipamorelin's ghrelin receptor activation produces synergistic GH release while preserving the natural pulsatile pattern that Sermorelin's short half-life generates; the two represent the physiological reference stack for researchers who want dual-receptor GH stimulation without engineered half-life extension. CJC-1295 DAC sits at the opposite pharmacokinetic extreme — week-long sustained GH elevation vs Sermorelin's brief physiological pulses; researchers studying the consequences of pulsatile vs sustained GH signaling on downstream IGF-1 production and tissue effects examine both as the endpoints of the GHRH analog kinetic spectrum. Tesamorelin uses the full 44-amino-acid GHRH sequence with a fatty acid N-terminal modification — the only other GHRH analog with prior FDA approval history, making it the natural regulatory and pharmacological reference compound alongside Sermorelin. GHRP-2 and GHRP-6 are ghrelin mimetics that researchers pair with Sermorelin when studying synergistic dual-receptor GH release using the most physiologically representative GHRH analog available.