GHRP-2 5mg
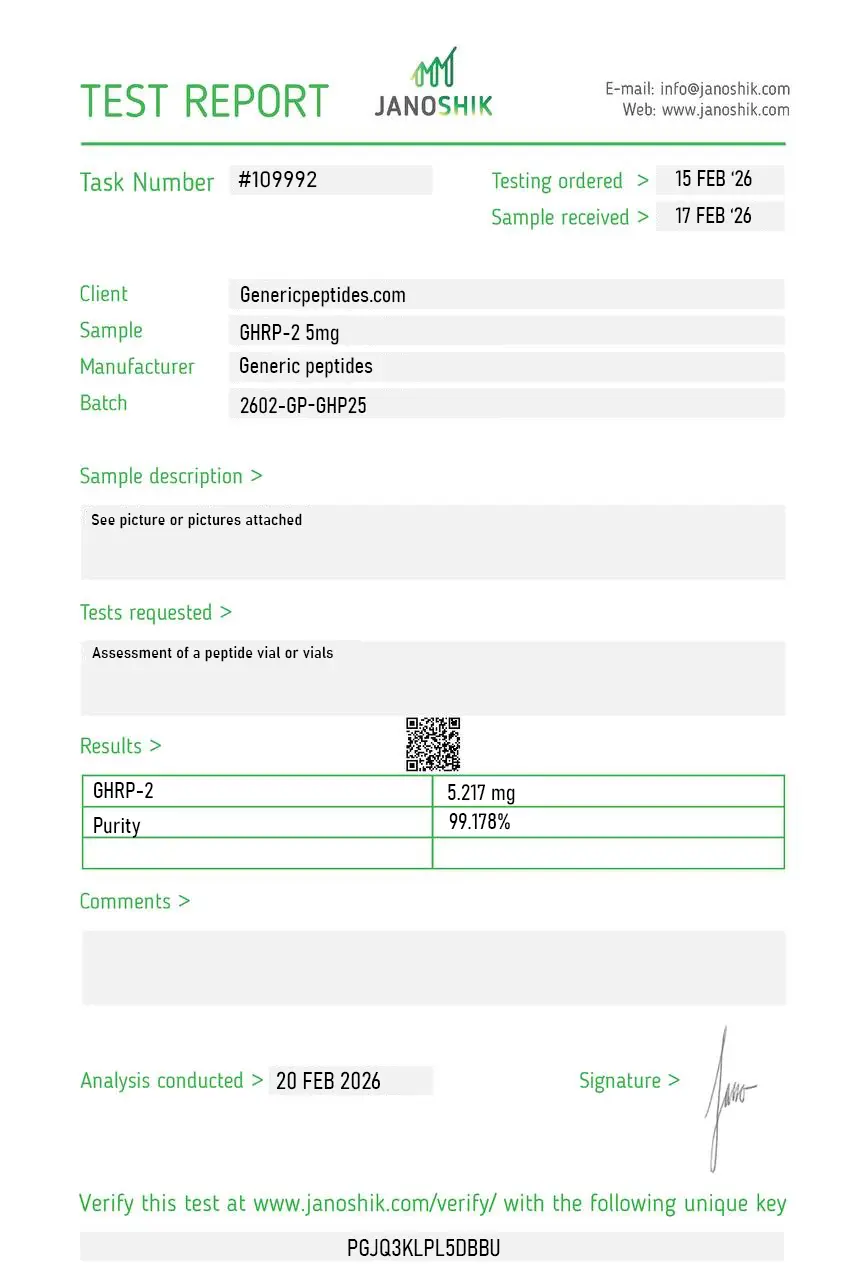
Certificate of Analysis available






Seven healthy men. One subcutaneous infusion of GHRP-2. They ate 36% more food at the buffet that followed than the saline group. Growth hormone shot up. Hunger followed. That 2005 Mount Sinai study established something blunt: GHRP-2 doesn't just stimulate GH release — it activates the same hunger circuit ghrelin runs through, which is exactly why it became one of the most-used research tools in appetite and GH biology.
GHRP-2 (Growth Hormone-Releasing Peptide-2) is a synthetic hexapeptide — six amino acids — that acts as a potent agonist of the ghrelin receptor (also called GHS-R1a, the growth hormone secretagogue receptor). Pralmorelin is its INN (International Nonproprietary Name), and KP-102 is what you'll see in older pharmaceutical literature.
Here's what makes it interesting: GHRP-2 mimics the body's natural ghrelin signal but with significantly stronger and more selective GH-releasing potency. Unlike GHRH (the hypothalamic hormone), GHRP-2 hits a completely different receptor pathway. That's the design feature that made it valuable as a research tool — and that's also why it became the go-to compound for studying ghrelin biology before more selective alternatives like Ipamorelin came along.
Researchers at the University of Turin published a head-to-head comparison in 1997 showing GHRP-2 stimulated GH secretion more effectively than GHRP-6, with relatively modest effects on prolactin, ACTH, and cortisol — though not zero. That comparative profile is what made GHRP-2 the second-generation GHRP that researchers actually preferred for clinical pharmacology work.
The appetite effect came later. The 2005 Mount Sinai infusion study (Laferrère et al., Journal of Clinical Endocrinology & Metabolism) was the first to confirm in humans that GHRP-2, like ghrelin itself, increases food intake — by 35.9% on average. That finding shifted GHRP-2 from being just a GH research tool to becoming a model for studying ghrelin's dual effects on growth hormone and feeding behavior. Both responses are real. Both are dose-dependent. Researchers have to design their protocols around them.
Here's the uncomfortable truth GHRP-2 marketing tends to skip: it's not a clean GH secretagogue the way Ipamorelin is. The 1997 comparative work showed GHRP-2 has measurable effects on cortisol, prolactin, and ACTH — minimal compared to GHRP-6, but real. For pure GH research without confounding hormonal noise, Ipamorelin is the cleaner tool. GHRP-2's value is specifically when researchers want strong GH release and want to study coordinated effects across the ghrelin axis — including appetite.
Regulatory note: GHRP-2 sits in an unusual regulatory position. It's currently in Category 3 on the FDA's interim 503A bulks list (insufficient evidence for evaluation) — different from the Category 2 group that recent attention has focused on. On the 503B outsourcing facility list, it's been in Category 1 specifically for non-injectable and non-nasal routes. WADA prohibits GHRP-2 for athletes in tested sports under the S2 category. As a research compound, it remains commercially available in the United States.
Here's a sourcing problem that's specific to GHRP-2: it's a six-amino-acid hexapeptide, which makes synthesis cheap and easy — but it's also a peptide where ratio integrity in the salt form matters for bioactivity. Most GHRP-2 sold online is the acetate salt, and cheap synthesis routinely produces inconsistent acetate content alongside peptide impurities and truncated sequences. With ghrelin receptor binding, sequence integrity is everything: even a single wrong residue can change receptor affinity dramatically, giving you a compound that looks like GHRP-2 but doesn't behave like it.
Generic Peptides supplies research-grade GHRP-2 for sale at 99% purity, manufactured in the USA. Domestic synthesis with verified hexapeptide sequence — the part that matters when receptor binding studies are the entire experiment.
Order GHRP-2 for sale in the USA — 99% purity, full hexapeptide sequence, manufactured domestically.
Yes — GHRP-2 is legally available as a research compound in the United States. It currently sits in Category 3 on the FDA's interim 503A bulks list (insufficient evidence for evaluation), so it cannot be compounded by traditional pharmacies. WADA prohibits it for tested athletes. Sales as a research compound continue legally.
Both target the ghrelin receptor (GHS-R1a), but Ipamorelin was specifically engineered to be more selective. GHRP-2 produces stronger absolute GH release but also measurable cortisol and prolactin effects. Ipamorelin's GH effect is somewhat smaller but cleaner from a side-effect standpoint. Different research tools for different design priorities.
Yes — that's confirmed. The 2005 Mount Sinai study in JCEM documented a 35.9% average increase in food intake during a buffet meal following GHRP-2 infusion. The appetite effect is one of the most reliably reproducible findings in GHRP-2 research and is a real consideration in any study design where feeding behavior is a confounding variable.
Yes — three names for the same molecule. Pralmorelin is the International Nonproprietary Name (INN). KP-102 was the original code name during pharmaceutical development. GHRP-2 is the most-used research name. CAS 158861-67-7 identifies the molecule unambiguously.
Probably not at the same purity. The hexapeptide is cheap to synthesize at low quality, which floods the market with budget product that has acetate inconsistencies, peptide impurities, or truncated sequences. The price gap reflects synthesis quality and verification, not pure markup.
Sources
Laferrère B et al. — "Growth Hormone Releasing Peptide-2 (GHRP-2), Like Ghrelin, Increases Food Intake in Healthy Men." Journal of Clinical Endocrinology & Metabolism, 2005. Documents the 35.9% food intake increase in human subjects. https://pubmed.ncbi.nlm.nih.gov/15699539/
Arvat E et al. — "Endocrine activities of growth hormone-releasing peptides." Comparative human pharmacology of GHRP-2 vs GHRP-6 from the University of Turin research group. Foundational work on relative selectivity. https://pubmed.ncbi.nlm.nih.gov/?term=arvat+ghrp-2
Bowers CY — "GH releasing peptides: structure and kinetics." Foundational research on GHRP family pharmacology and ghrelin receptor agonism. https://pubmed.ncbi.nlm.nih.gov/8500634/
FDA — "Bulk Drug Substances Nominated for Use in Compounding Under Section 503A," updated April 22, 2026. Documents GHRP-2 Category 3 status on the interim 503A bulks list. https://www.fda.gov/media/94155/download
Hexapeptide. One sequence that has to be exact. 99% purity, USA-made.
GHRP-2 (pralmorelin) ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its hexapeptide structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — GHRP-2 contains a tryptophan residue that's particularly prone to photodegradation. | Always keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | The tryptophan residue also makes GHRP-2 susceptible to oxidation if the vial seal is broken or the powder is exposed to air. | Keep the aluminum crimp cap intact until ready to reconstitute. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
Independent lab test reports are available for GHRP-2 5mg and 10mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.
Pralmorelin. KP-102. Whatever you call it, the diagnostic-test heritage in Japan is the interesting part — it got used clinically as a GH stimulation test, safer than the insulin-tolerance approach for pediatric assessment. We reference that lineage in our protocol design. Material's been steady.
Honestly bought it as the dirty comparator. We run a clean-versus-dirty GHRP contrast and GHRP-2 is the dirty one — full corticotropic spillover. It performs that role reliably, which is all I need from it.
Decent. One thing: GHRP-2 produces a stronger GH response per dose than GHRP-6 but a weaker appetite signal — opposite balance to its sibling — and people swap them assuming equivalence. They aren't. We dose each separately. The compound was reliable; the family-level confusion is just a field-wide hazard.
Reorder, fourth one I think. Somatotroph assays. No drama.
What I appreciate is they don't bundle it into a "stack" pitch. GHRP-2 hits the ghrelin receptor, CJC hits GHRH-R, they're different mechanisms, and seeing them kept separate instead of sold as a combo tells me whoever wrote the listing actually understands the pharmacology.
Decent. One thing: GHRP-2 produces a stronger GH response per dose than GHRP-6 but a weaker appetite signal — opposite balance to its sibling — and people swap them assuming equivalence. They aren't. We dose each separately. The compound was reliable; the family-level confusion is just a field-wide hazard.
Used it in anti-doping method-development work — it's a WADA-prohibited secretagogue, so we need authentic reference material to build the LC-MS detection assays around. The COA actually noted the prohibited status, which is unusual and convenient for our audit trail. Material matched our existing standard.
Reconstituted clean, no precipitate, behaved across our dose range. We measure the cortisol and prolactin alongside GH specifically because GHRP-2 moves all three — that off-target profile is our actual readout, not a side issue. Held up.
Bowers' GHRP family work is the foundation and GHRP-2 was one of the more potent ones to come out of it. We reference the original characterization in our methods. The material's been consistent enough that batch variability hasn't entered our error analysis.
GHRP-2 binds to the ghrelin receptor (GHS-R1a) on pituitary somatotrophs and hypothalamic neurons, triggering Gq-coupled signaling that drives calcium influx and downstream GH release. It hits a completely different receptor than GHRH analogs do — that's why combining a GHRH analog with a GHRP produces synergistic GH release rather than additive effects.
GHRP-6 was the first-generation peptide; GHRP-2 was developed as an improvement. GHRP-2 produces stronger GH release per dose with relatively less appetite stimulation than GHRP-6 (which is notorious for hunger effects). Both still increase appetite in humans, but GHRP-6's effect is more pronounced.
Yes — modestly. The 1997 Turin comparative research documented that GHRP-2 has measurable effects on cortisol, prolactin, and ACTH, though smaller than GHRP-6. Researchers needing pure GH stimulation without these confounders typically choose Ipamorelin instead, which is more selective for the ghrelin receptor without significant off-target hormonal activation.
The hexapeptide is one of the easier peptides to synthesize at low quality, so the budget end of the market is flooded with product containing peptide impurities, truncated sequences, or inconsistent acetate content. Cheap GHRP-2 looks identical on a label to high-purity material. The bioactivity differences only show up in receptor binding assays.
GHRP-2 was developed in the late 1980s and early 1990s by Cyril Bowers' group, building on earlier GHRP-6 research. It was initially investigated under the code name KP-102, and the Turin clinical pharmacology group established its comparative profile in the mid-1990s. The compound has nearly four decades of research literature behind it.
Yes. WADA prohibits GHRP-2 for athletes subject to drug testing under category S2 (Peptide Hormones, Growth Factors, Related Substances). The classification covers all GHRPs and growth hormone secretagogues — GHRP-2 is named explicitly. Athletes in tested sports should avoid it regardless of how it's obtained.
Pralmorelin (the International Nonproprietary Name), KP-102 (the original development code), and GHRP-2 (the most common research name). CAS number 158861-67-7. The salt form most commonly sold is GHRP-2 acetate. All four names refer to the same hexapeptide.
Growth hormone axis pharmacology and ghrelin receptor signaling lead by volume. There's also active work in appetite regulation and feeding behavior research — the 2005 JCEM paper opened a substantial line of investigation. GHRP-2 has also been used in cardiology research for cardioprotective signaling and in pediatric endocrinology for GH deficiency diagnosis.
Both target the ghrelin receptor, but they're structurally different. GHRP-2 is a peptide; Ibutamoren is an orally bioavailable small molecule. Ibutamoren has a much longer half-life (~24 hours vs GHRP-2's hours) and produces sustained GH elevation rather than pulses. Different research tools for chronic vs acute exposure designs.
Native ghrelin requires post-translational modification (octanoylation) to be active and degrades rapidly in circulation. GHRP-2 was engineered to be stable, potent, and synthesizable without the lipid modification. It also crosses the blood-brain barrier more readily than ghrelin itself, which matters for any research targeting central GHS-R1a populations.
Researchers investigating ghrelin mimetics and growth hormone secretagogue pharmacology consistently examine GHRP-2 alongside compounds that target the GH axis through related or complementary receptor pathways. GHRP-6 is the most direct comparison — both are hexapeptide ghrelin mimetics with similar GH-releasing potency, but GHRP-6 produces stronger appetite stimulation through ghrelin receptor activity in hypothalamic feeding circuits while GHRP-2 has a somewhat cleaner side effect profile; researchers studying ghrelin receptor selectivity typically examine both in parallel. Ipamorelin is the third ghrelin mimetic in the comparison set — weaker GH pulse than GHRP-2 but with minimal cortisol, prolactin, and appetite off-target activity, making it the preferred selectivity reference compound. Hexarelin produces the strongest GH release of any ghrelin mimetic currently available and is examined alongside GHRP-2 in potency comparison research. Mod GRF (1-29) is consistently paired with GHRP-2 in research designs targeting synergistic dual-receptor GH release — GHRH receptor plus ghrelin receptor activation on the same pituitary somatotrophs produces substantially greater GH output than either compound alone.