CJC-1295 2mg
Certificate of Analysis available






Native GHRH has a half-life of about 7 minutes. By the time you finish saying the word "growth," most of the molecule is already cleaved by the enzyme dipeptidyl peptidase-4. ConjuChem's chemists in the early 2000s asked the obvious question: what if we change four amino acids and make the molecule resistant to that enzyme? They got Modified GRF 1-29 — a peptide with the same GHRH receptor activity but a 30-minute half-life. Same biology, different pharmacology.
Modified GRF (1-29), also called CJC-1295 without DAC, is a synthetic 29-amino-acid GHRH analog. It's the first 29 residues of natural GHRH — the active fragment — with four targeted amino acid substitutions (D-Ala at position 2, Gln at position 8, Ala at position 15, Leu at position 27) that resist enzymatic degradation. Same active site that binds the GHRH receptor on pituitary somatotrophs. Just engineered for stability.
The "DAC" terminology gets confusing fast. CJC-1295 is the same modified 29-amino-acid peptide. CJC-1295 with DAC adds a Drug Affinity Complex tag (a maleimidopropionic acid derivative) that binds to serum albumin and extends half-life from 30 minutes to 6-8 days. Mod GRF (1-29) is the same molecule without that DAC tag — engineered for resistance to enzymatic cleavage but lacking the albumin-binding extension. Two different research tools made from the same modified backbone.
Why would researchers choose Mod GRF (1-29) over CJC-1295 DAC? Because GHRH is supposed to act in pulses, not continuous waves. The natural pituitary releases GH in discrete bursts, several times a day, in response to pulsatile hypothalamic GHRH signaling. CJC-1295 DAC's 6-8 day half-life flattens that pulsatile pattern into a sustained baseline elevation — useful for some research designs, fundamentally non-physiological for others.
Mod GRF (1-29)'s 30-minute half-life preserves the pulsatile signaling pattern. Researchers studying coordinated GH release pair it with Ipamorelin or another ghrelin mimetic, where the matching short half-lives produce simultaneous pulses through both receptor pathways. This is why Mod GRF (1-29) is the GHRH component in the most-prescribed GH peptide stack — its kinetics match the ghrelin mimetics' kinetics. A DAC-tagged version doesn't.
Here's what the marketing pages don't always make clear: Mod GRF (1-29) is essentially the same backbone as Sermorelin with the four stability substitutions added. Sermorelin is unmodified GRF 1-29 — FDA-approved for pediatric GH deficiency before being voluntarily discontinued in 2008. Tesamorelin (Egrifta) is a different GHRH analog with a trans-3-hexenoic acid modification, FDA-approved for HIV-associated lipodystrophy. All three target the same receptor. Their pharmacokinetics differ.
The honest part: Mod GRF (1-29)'s human research literature is thinner than CJC-1295 DAC's, partly because most clinical trials used the longer-acting DAC version. Animal data and short-term human pharmacokinetic studies support the mechanism. Long-term outcome data on the no-DAC version specifically is limited.
Regulatory note: CJC-1295 (free base, acetate) and CJC-1295 with DAC variants were placed on the FDA's Category 2 bulks list in 2023. Both versions were removed from Category 2 on September 27, 2024 after the original nominations were withdrawn. The PCAC reviewed CJC-1295 at its December 4, 2024 meeting and voted against Category 1 inclusion. As of May 2026, Mod GRF (1-29) / CJC-1295 (no DAC) sits in regulatory limbo — not in Category 2, not in Category 1, ineligible for 503A compounding pharmacy production. WADA prohibits it for athletes in tested sports.
Here's a sourcing problem that's specific to Mod GRF (1-29): cheap suppliers routinely sell Sermorelin (unmodified GRF 1-29) labeled as Mod GRF (1-29), or sell partially modified material with only some of the four amino acid substitutions correctly incorporated. The four stability substitutions are the entire reason this peptide exists — without them, you have Sermorelin's half-life of about 11 minutes rather than Mod GRF's 30 minutes. Detection requires HPLC-MS analysis specifically targeting the modified residue positions. Most budget suppliers don't run that verification, which means the price gap often reflects whether the substitutions are actually there.
Generic Peptides supplies research-grade Mod GRF (1-29) for sale at 99% purity, manufactured in the USA. Domestic synthesis with all four amino acid substitutions verified — the part that determines whether you have Mod GRF or accidentally-purchased-Sermorelin pharmacology.
Order Mod GRF (1-29) for sale in the USA — 99% purity, all four substitutions verified, manufactured domestically.
Yes — Mod GRF (1-29) / CJC-1295 (no DAC) is legally available as a research compound in the United States. It was removed from FDA Category 2 in September 2024, but the PCAC voted against Category 1 inclusion at its December 2024 meeting, so it cannot currently be compounded by 503A pharmacies. Sales as a research compound continue legally. WADA prohibits it for tested athletes.
Same modified 29-amino-acid backbone, but CJC-1295 DAC adds a maleimidopropionic acid tag that binds serum albumin and extends half-life from 30 minutes to 6-8 days. Mod GRF (1-29) preserves pulsatile GH release; CJC-1295 DAC produces sustained baseline elevation. Different research tools depending on whether physiological pulse patterns or chronic exposure is the experimental target.
Related but distinct. Sermorelin is unmodified GRF 1-29 with a half-life of about 11 minutes. Mod GRF (1-29) has four amino acid substitutions (D-Ala-2, Gln-8, Ala-15, Leu-27) that resist enzymatic cleavage, extending half-life to about 30 minutes. Same active sequence, different stability. Cheap suppliers often sell Sermorelin labeled as Mod GRF — verify the substitutions are present.
Because their half-lives match. Both are short-acting (30 minutes for Mod GRF, ~2 hours for Ipamorelin) and produce pulsatile signaling rather than sustained elevation. They target different receptors (GHRH receptor vs ghrelin receptor) on the same pituitary cells, so combining them produces synergistic GH release while preserving the pulse pattern. CJC-1295 DAC paired with Ipamorelin would smear the pulse into a flat baseline — defeating the purpose.
Probably not at the same purity or with all four substitutions intact. The amino acid substitutions are the technically demanding, expensive part of the synthesis. Cheap suppliers routinely sell unmodified Sermorelin under the Mod GRF label, or material with only partial substitution. Without HPLC-MS verification of each modified position, the difference is invisible until your half-life data doesn't match published research.
Sources
Teichman SL et al. — "Prolonged stimulation of growth hormone (GH) and insulin-like growth factor I secretion by CJC-1295." Journal of Clinical Endocrinology & Metabolism, 2006. Documents CJC-1295 receptor pharmacology and the modifications shared with the no-DAC version. https://pubmed.ncbi.nlm.nih.gov/16352683/
Alba M et al. — "Once-daily administration of CJC-1295, a long-acting GHRH analog, normalizes growth in the GHRH knockout mouse." American Journal of Physiology - Endocrinology and Metabolism, 2006. Foundational pharmacology research on CJC-1295's modified backbone. https://journals.physiology.org/doi/full/10.1152/ajpendo.00201.2006
Lexology — "FDA removes certain peptide bulk drug substances from Category 2." Industry analysis of the September 2024 reclassification including CJC-1295 free base, acetate, and DAC variants, plus the December 4, 2024 PCAC review outcome. https://www.lexology.com/library/detail.aspx?g=2e55b76a-3173-4e04-beda-bf021202f18d
FDA — "Bulk Drug Substances Nominated for Use in Compounding Under Section 503A," updated April 22, 2026. Documents CJC-1295 / Mod GRF (1-29) regulatory status and PCAC review outcomes. https://www.fda.gov/media/94155/download
Four substitutions. One pulse pattern. Sourcing determines whether you have Mod GRF or Sermorelin in disguise.
Mod GRF (1-29), also known as CJC-1295 no DAC, ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its modified GHRH structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — protect from direct light and UV exposure to prevent photodegradation. | Keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a frost-free freezer with temperature swings, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
<
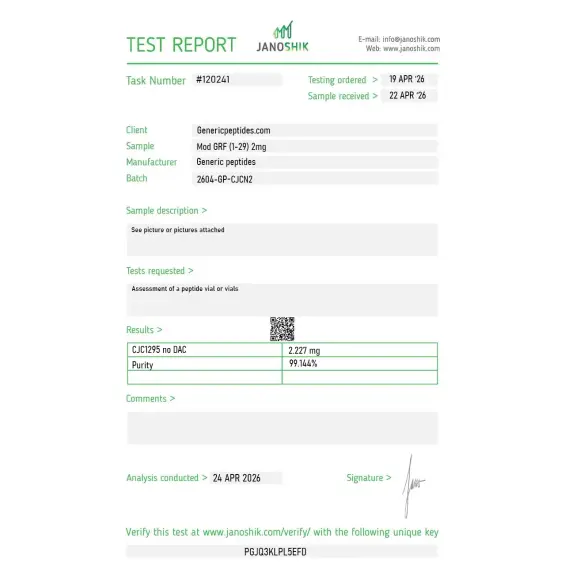
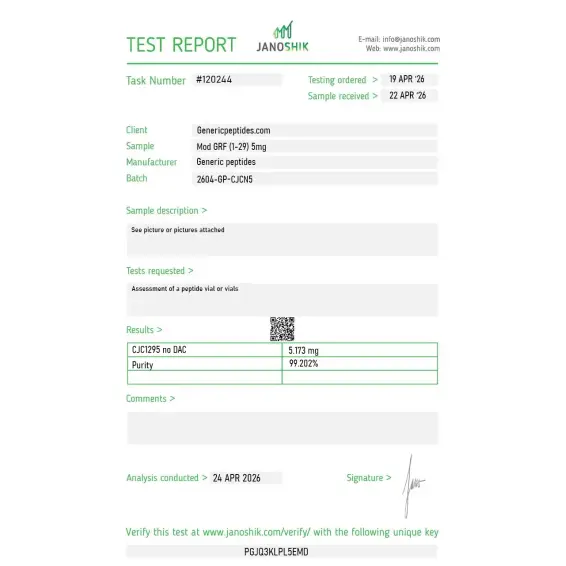
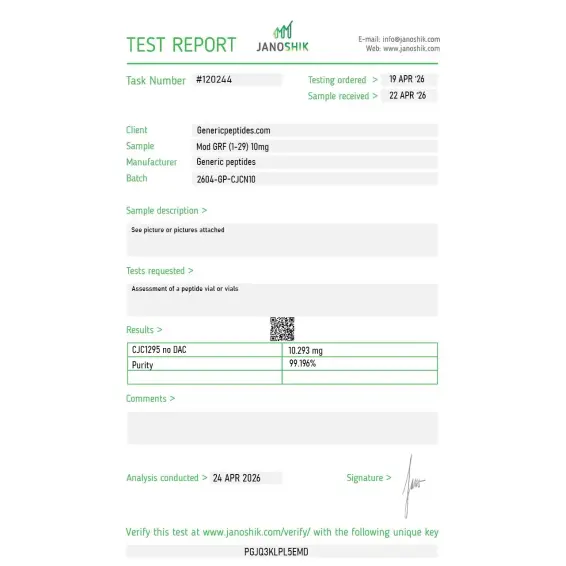
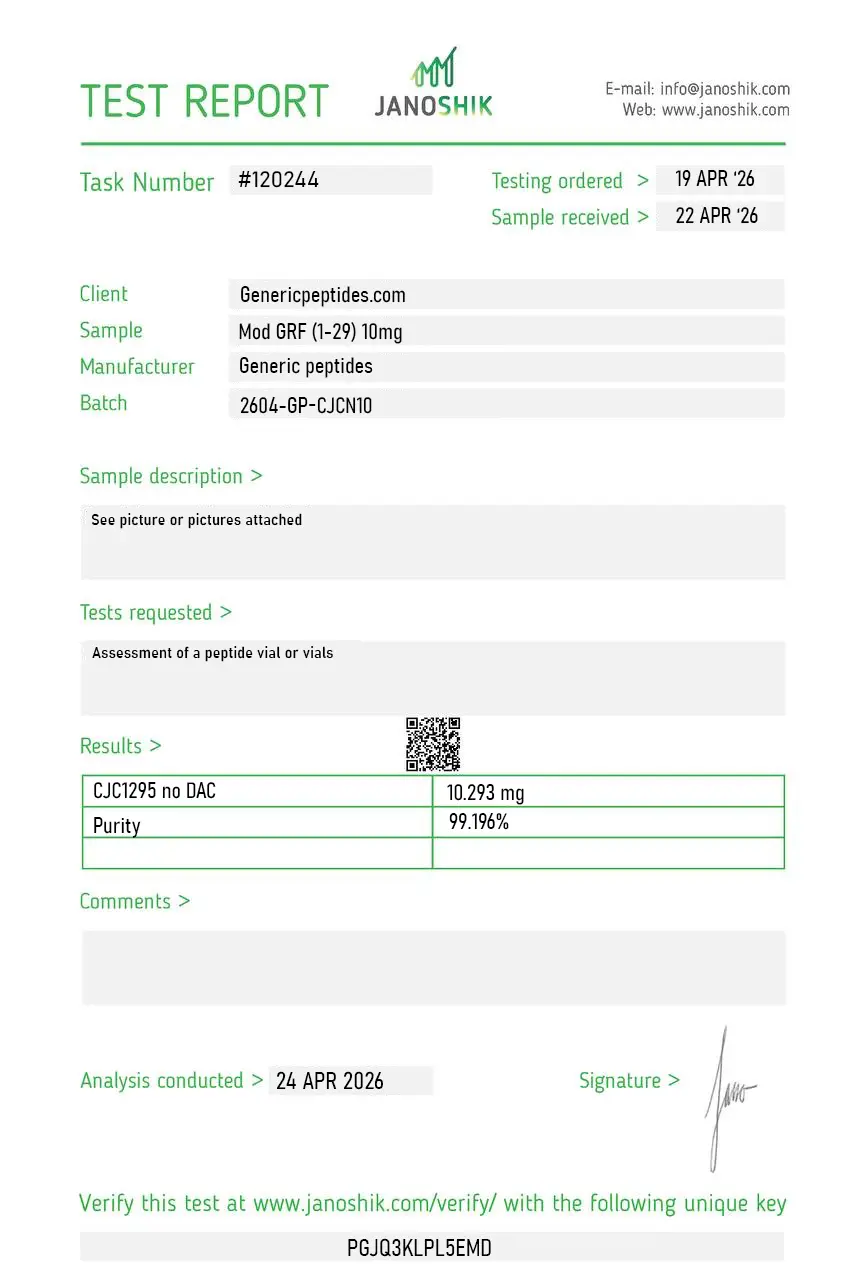
Independent lab test reports are available for CJC-1295 2mg, 5mg, and 10mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

p>
The single most important thing about ordering this compound is confirming it's the No-DAC version and not CJC-1295 DAC — they get sold under overlapping names and have completely different half-lives, thirty minutes versus about a week. This vendor labels it clearly. Star off because the molecular weight on the COA is the surest way to tell them apart and it wasn't prominently stated.
The four substitutions are the whole point — D-Ala at position 2 to block DPP-IV, the others to stop deamidation and oxidation. Gives you a stabilized GRF(1-29) that survives extended in-vitro incubation where native sermorelin would degrade. Used it for exactly that in somatotroph signaling work. Consistent.
ConjuChem developed this as the tetrasubstituted base before they added the DAC linker to make the long-acting version — so Mod GRF is essentially the intermediate that never went into serious clinical trials on its own. That history clarifies why the published data is thin for this exact compound. The listing acknowledges it. Material activated the receptor as expected.
We anchor a structure-activity series with this — native sermorelin, then the tetrasubstituted Mod GRF, then the DAC version, then tesamorelin. Mod GRF is the "stabilized but still pulsatile" point on that spectrum. Each modification's effect on receptor kinetics only makes sense with the others present. Material slotted in without a vendor artifact.
For comparing pulsatile against sustained GHRH-receptor activation, Mod GRF is the pulsatile arm and the DAC version is the sustained arm. Sourcing both from one place with matched documentation is what makes that kinetic comparison clean. The thirty-minute versus week-long half-life contrast is the entire experiment, and vendor variability would muddy it.
The DPP-IV-resistance engineering here is the same logic that runs through the modern incretin drugs — the D-Ala-2 trick to dodge the same protease. Working with Mod GRF as a GHRH example helps frame why that protection strategy is so widespread across peptide drug design. Material behaved as the pharmacology predicts.
Tetrasubstituted GRF(1-29) as our stabilized-pulsatile GHRH reference. Consistent batches, repeated orders. That's it.
Performs in somatotroph assays. Practical note: even with the four stabilizing substitutions it's still a pulsatile-kinetics compound, not long-acting — if your protocol assumed sustained activation you want the DAC version instead. We confirmed the right choice for our pulsatile design. Material was fine; just match the compound to your kinetic question.
The peptide binds GHRH receptors on somatotroph cells in the anterior pituitary, activating adenylyl cyclase and triggering the cAMP-PKA cascade that drives GH gene transcription and release. It works upstream — telling the pituitary to make and release more of its own GH rather than supplying GH directly. The modification preserves this receptor binding while making the molecule resistant to dipeptidyl peptidase-4 cleavage.
Both are GHRH analogs targeting the same receptor with engineered stability modifications. Mod GRF (1-29) has four amino acid substitutions producing a 30-minute half-life. Tesamorelin has a single trans-3-hexenoic acid modification at the N-terminus producing a different stability profile — and it's FDA-approved for HIV-associated lipodystrophy. Different engineering strategies, different regulatory pathways.
The four amino acid substitutions specifically target the cleavage sites used by dipeptidyl peptidase-4 (DPP-4) and other peptidases that rapidly degrade native GHRH. D-Ala at position 2 alone provides significant DPP-4 resistance; the additional substitutions at positions 8, 15, and 27 protect against other enzymatic pathways. Together they produce roughly a 4-fold half-life extension.
The four amino acid substitutions are the technically demanding, expensive part of the synthesis. Cheap suppliers routinely sell unmodified Sermorelin (which has only the natural GRF 1-29 sequence) under the Mod GRF label, or produce material with only partial substitution. HPLC-MS analysis specifically targeting each modified position is required to verify all four substitutions are present.
The modified GRF backbone was developed by ConjuChem, a Canadian biotech, in the early 2000s as part of their CJC-1295 program. The four amino acid substitutions were established in the 2002-2006 timeframe, with the foundational human pharmacokinetic paper published by Teichman in 2006. The same modified backbone is used in CJC-1295 with and without DAC.
Yes. WADA prohibits CJC-1295 (with or without DAC) under category S2 (Peptide Hormones, Growth Factors, Related Substances). The classification covers the modified GRF backbone regardless of DAC status. Athletes subject to drug testing should avoid the compound regardless of how it's obtained.
CJC-1295 (no DAC), CJC-1295 free base, CJC-1295 acetate, Modified GRF 1-29, Mod GRF, and the chemical descriptor [D-Ala²,Gln⁸,Ala¹⁵,Leu²⁷]GRF(1-29). All names refer to the same modified 29-amino-acid peptide. The DAC variants are separate compounds.
Growth hormone axis pharmacology and pulsatile GH release research lead by volume. The peptide is particularly used in combination protocols with Ipamorelin or other ghrelin mimetics, where matched short half-lives produce coordinated pulses through both receptor pathways. There's also research in body composition, recovery, and aging-related GH decline using the modified GRF backbone as a research tool.
Pulse pattern preservation. Mod GRF (1-29)'s 30-minute half-life allows for pulsatile GH release that mimics natural physiology, while CJC-1295 DAC's 6-8 day half-life produces sustained baseline elevation. Researchers studying physiological GH patterns or combining with short-acting ghrelin mimetics need the no-DAC version. The DAC version is for chronic-exposure research designs.
The four amino acid substitutions provide enzymatic stability without changing the active receptor-binding region. Natural GHRH has a 7-minute half-life and produces brief, immediate GH pulses. Mod GRF (1-29) has a 30-minute half-life producing somewhat extended pulses while preserving the receptor pharmacology. The modifications are specifically designed to extend duration without altering the biological signal.
Researchers investigating GHRH receptor pharmacology and pulsatile growth hormone release consistently examine Mod GRF (1-29) alongside compounds that target the GH axis through complementary receptor pathways or contrasting stability profiles. Ipamorelin is the defining pairing — Mod GRF activates the GHRH receptor while Ipamorelin activates the ghrelin receptor on the same pituitary somatotrophs; their matching 30-minute half-lives produce synchronized dual-receptor GH pulses, which is why this combination is the most-studied GH peptide stack in the research literature and why the two compounds are almost always examined together. CJC-1295 DAC is the direct pharmacokinetic comparison — same modified 29-amino-acid backbone but with the DAC albumin-binding tag extending half-life from 30 minutes to 6-8 days; researchers studying pulsatile vs sustained GH release patterns examine both to isolate the pharmacokinetic contribution of the DAC modification independent of receptor biology. Sermorelin is the unmodified GRF 1-29 reference — identical active sequence without the four stability substitutions, useful when researchers need to isolate the pharmacological contribution of the amino acid modifications that define Mod GRF. GHRP-2 and GHRP-6 are ghrelin mimetics that researchers substitute for Ipamorelin when studying how different ghrelin receptor activation profiles interact with GHRH receptor signaling.