Hexarelin 2mg
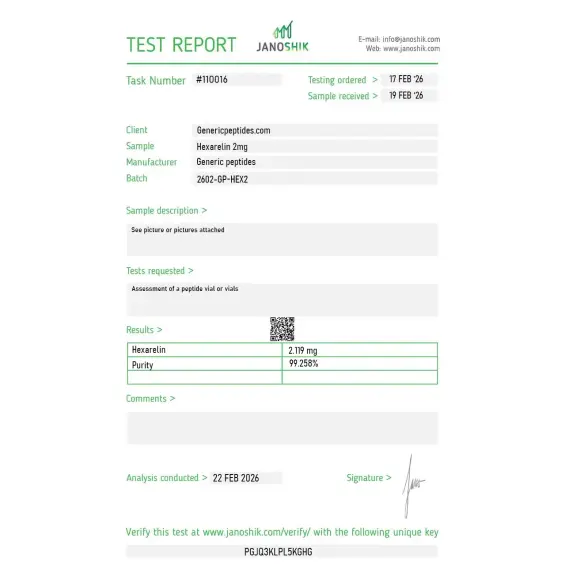
Certificate of Analysis available





Italian researchers ran a 1999 experiment that should have ended a long debate about how growth hormone–releasing peptides actually work. They surgically removed the pituitary glands from rats — meaning the animals couldn't release growth hormone at all — then induced cardiac ischemia. Hexarelin still protected the heart. No GH was being released. Whatever was happening, it wasn't going through the growth hormone pathway. That experiment forced the field to admit Hexarelin was doing something nobody had fully mapped yet.
Hexarelin is a synthetic hexapeptide — six amino acids — engineered as a more potent analog of GHRP-6. Its name says it directly: hexa (six) plus (gh)relin. It's the most potent growth hormone–releasing peptide in the GHRP family, producing roughly a 30-fold increase in GH secretion compared to baseline in published research, surpassing GHRP-2 and GHRP-6 in raw stimulation strength.
What makes Hexarelin genuinely different from the other GHRPs isn't the GH release. It's the second receptor: CD36, a scavenger receptor expressed densely in cardiac tissue. Hexarelin binds GHS-R1a (the ghrelin receptor) like other GHRPs, but it also binds CD36 — and the cardiac effects observed in research appear to come primarily through CD36, independent of growth hormone entirely.
The landmark 1994 paper from Ezio Ghigo's group at the University of Turin (Journal of Clinical Endocrinology & Metabolism) established Hexarelin's pharmacology in humans. They tested intravenous, subcutaneous, intranasal, and oral administration. Hexarelin was active by every route — including oral, which is unusual for a peptide. The GH-releasing potency dwarfed anything in the GHRP family at the time.
The Locatelli 1999 hypophysectomized rat experiment is what changed the story. By removing the pituitary, researchers eliminated GH release as a confound. Hexarelin still prevented cardiac ischemia-reperfusion damage. CD36 receptor binding turned out to be the explanation. That dual-pathway mechanism — GH release through GHS-R1a, cardioprotection through CD36 — is why Hexarelin became a unique research tool in cardiovascular biology, not just endocrinology.
The uncomfortable truth Hexarelin marketing tends to skip: receptor desensitization is a real problem. The intense GHS-R1a stimulation that makes Hexarelin so potent also causes faster receptor downregulation than milder GHRPs. Repeated exposure leads to diminishing GH responses within weeks. For research designs requiring sustained pharmacological GH stimulation, that's a fundamental constraint. It's why short-cycle research protocols dominate the literature — Hexarelin is a tool for acute and short-term studies, not chronic ones.
It's also not "clean" the way Ipamorelin is. Hexarelin produces measurable cortisol and prolactin elevation alongside GH release, similar to GHRP-2 but more pronounced. For research focused on isolated GH biology without confounding hormones, Ipamorelin is the cleaner choice. Hexarelin's value is specifically when researchers need maximum GH stimulation, when they're studying CD36-mediated cardiac signaling, or when they're using it as a diagnostic tool to test pituitary GH reserve.
Regulatory note: Hexarelin is not separately listed on the FDA's 503A bulks list as of May 2026. It's not in Category 2 with the BPC-157 / Epitalon / DSIP group, but it's also not approved for compounding under any current pathway. WADA prohibits Hexarelin for athletes in tested sports under category S2 (Peptide Hormones, Growth Factors, Related Substances, and Mimetics) — at all times, in and out of competition. As a research compound, it remains commercially available.
Here's a sourcing problem that's specific to Hexarelin: it contains a methyltryptophan residue that distinguishes it from GHRP-6 and gives it the cardiac receptor affinity that defines its profile. That modified amino acid is harder to incorporate cleanly during synthesis — cheap production routinely uses unmodified tryptophan or fails to verify the methylation, producing material that's structurally closer to GHRP-6 than to actual Hexarelin. The compound that arrives in your vial may be the right molecular weight on paper but won't bind CD36 the way the literature describes. Without HPLC-MS verification specifically checking the methyltryptophan position, this defect is invisible to buyers.
Generic Peptides supplies research-grade Hexarelin for sale at 99% purity, manufactured in the USA. Domestic synthesis with verified methyltryptophan incorporation — the part that determines whether you're studying Hexarelin pharmacology or accidentally studying GHRP-6 pharmacology with the wrong label.
Order Hexarelin for sale in the USA — 99% purity, methyltryptophan verified, manufactured domestically.
Yes — Hexarelin is legally available as a research compound in the United States. It's not on the FDA's 503A bulks list for compounding eligibility, and it's not in Category 2 with the recent regulatory activity. Not FDA-approved for human use. WADA prohibits it for tested athletes in all categories.
Hexarelin is essentially GHRP-6 with a methyltryptophan modification that increases potency, stability, and CD36 receptor affinity. Hexarelin produces stronger GH release and adds the cardioprotective CD36 pathway. GHRP-6 is the parent compound; Hexarelin is the optimized successor.
The intensity of GHS-R1a activation triggers faster receptor downregulation than milder agonists like Ipamorelin. The very potency that makes Hexarelin valuable also limits its sustained use. Research protocols typically use short cycles to minimize tachyphylaxis effects.
Yes — that's what makes it pharmacologically interesting. The 1999 Locatelli hypophysectomized rat study demonstrated cardioprotective effects in animals incapable of releasing GH. The mechanism involves CD36 receptor binding on cardiomyocytes, not just GHS-R1a-mediated GH release. This dual pathway is unique among the GHRPs.
Probably not. The methyltryptophan residue requires specialized synthesis steps that cheap production routinely skips, producing material structurally similar to GHRP-6 but mislabeled as Hexarelin. Without analytical verification of the modified residue, the difference is invisible — until your CD36 binding assay produces nothing.
Sources
Ghigo E, Arvat E, Gianotti L et al. — "Growth hormone-releasing activity of hexarelin, a new synthetic hexapeptide, after intravenous, subcutaneous, intranasal, and oral administration in man." Journal of Clinical Endocrinology & Metabolism, 1994;78(3):693-698. The landmark human pharmacology study. https://pubmed.ncbi.nlm.nih.gov/8126144/
Locatelli V et al. — Cardioprotective effects of Hexarelin in hypophysectomized rats demonstrating GH-independent activity. The foundational research establishing the CD36 pathway. https://pubmed.ncbi.nlm.nih.gov/10465272/
"The cardiovascular action of hexarelin." PMC, 2014. Comprehensive review of cardiovascular research and CD36 receptor pharmacology. https://pmc.ncbi.nlm.nih.gov/articles/PMC4178518/
WADA — "Prohibited List" 2025. Documents Hexarelin classification under category S2 for tested athletes. https://www.wada-ama.org/en/prohibited-list
The strongest GHRP. Two receptors. One modified residue that has to be exactly right.
Hexarelin ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its hexapeptide structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — Hexarelin contains two tryptophan residues that are particularly prone to photodegradation. | Always keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | The two tryptophan residues also make Hexarelin susceptible to oxidation if the vial seal is broken or the powder is exposed to air. | Keep the aluminum crimp cap intact until ready to reconstitute. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
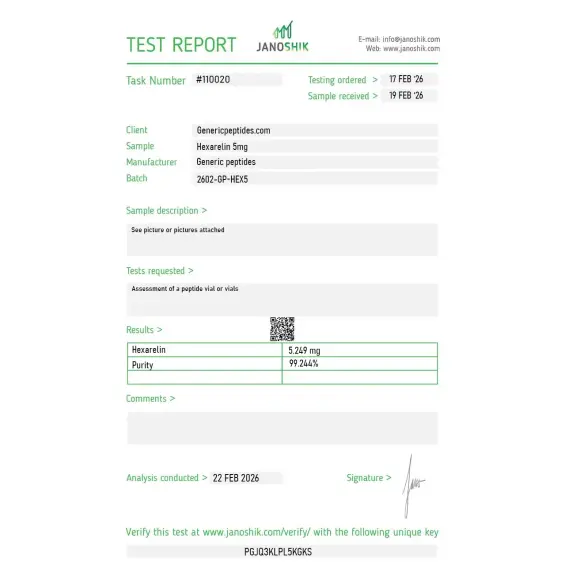
Independent lab test reports are available for Hexarelin 2mg and 5mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

Deghenghi developed this at Mediolanum in Italy in the early nineties, and most of the published clinical literature still traces to those Italian endocrinology groups. Nice that the listing references that development origin. Material gave consistent activation in our receptor work.
The rapid GHS-R1a desensitization is the defining experimental constraint — Hexarelin downregulates the receptor fast on repeated exposure, so your dosing schedule determines whether you're studying acute activation or desensitization. The listing actually flags that, which most don't. We designed our protocol around it and the material behaved predictably.
Decent for our cardiac pharmacology work. The CD36 angle is underappreciated — most people buy Hexarelin thinking GH release and miss that the cardiomyocyte effects run through a completely separate scavenger receptor. For our infarct-model signaling work that's the entire point. Material was reliable; I just wish the listing developed the CD36 mechanism more, since it's what distinguishes the compound.
The Phase II clinical history is useful context — Hexarelin had the strongest acute GH response of the GHRPs but the desensitization killed sustained therapeutic application, which is why it never reached approval despite strong early data. The listing acknowledging that failure mode rather than implying clinical success is the honest framing. Material consistent.
For comparative GHRP pharmacology we run all four — GHRP-2, GHRP-6, Hexarelin, Ipamorelin — and Hexarelin is the one with the extra CD36 dimension the others lack, plus the strongest acute GH potency. Sourcing the family from one place keeps the comparison interpretable. That dual-receptor outlier status is what makes Hexarelin distinct in the set.
The methyl-tryptophan modification is the structural elegance — that single methylation at position 2 gives Hexarelin enzymatic stability and the distinct receptor profile versus GHRP-2. Mass spec showing the expected plus-fourteen shift relative to GHRP-2 confirms you've got the right compound. Material was consistent with that signature.
Dual-receptor GHRP as our cardiac-signaling reference. Consistent batches, repeated orders. Covers it.
Hexarelin binds GHS-R1a (the ghrelin receptor) on pituitary somatotrophs and hypothalamic neurons, activating Gq-coupled signaling and downstream calcium influx that drives GH release. The intensity of GHS-R1a activation is higher than other GHRPs, producing the strongest absolute GH release in the family — roughly 30-fold over baseline in published research. The cost is faster receptor desensitization with repeated exposure.
Both target GHS-R1a, but their selectivity profiles are very different. Ipamorelin was engineered for clean GH release without significant cortisol, prolactin, or appetite effects. Hexarelin produces stronger GH release but with measurable off-target hormonal activation. Ipamorelin also doesn't engage CD36 — Hexarelin's secondary receptor that drives its cardiac effects.
CD36 is a scavenger receptor expressed densely in cardiac tissue and elsewhere. Hexarelin binds CD36 with significant affinity, which explains its cardioprotective effects in research models — including the GH-independent cardioprotection observed in hypophysectomized animals. CD36 binding makes Hexarelin pharmacologically distinct from every other GHRP.
The peptide contains a methyltryptophan residue at position 2 that distinguishes it from GHRP-6 and is essential for its receptor profile. Cheap synthesis routinely substitutes regular tryptophan or fails to verify the methylation, producing material that's effectively GHRP-6 mislabeled as Hexarelin. Detection requires HPLC-MS analysis specifically targeting the modified residue.
Hexarelin was developed in the early 1990s by Romano Deghenghi's group at Mediolanum Farmaceutici, building on GHRP-6's structure-activity work. The 1994 Ghigo human pharmacology paper established its clinical profile. The cardiac mechanism research expanded through the late 1990s and 2000s, particularly through Italian and Canadian research groups.
Yes. WADA prohibits Hexarelin for athletes subject to drug testing under category S2 — Peptide Hormones, Growth Factors, Related Substances, and Mimetics. The classification covers all GHRPs and growth hormone secretagogues, with Hexarelin specifically named in WADA literature. Athletes in tested sports should avoid it regardless of how it's obtained.
Hexarelin Acetate, HEX, Examorelin (older designation), and the chemical descriptor His-D-2-methyl-Trp-Ala-Trp-D-Phe-Lys-NH₂. CAS number 140703-51-1 for the free peptide. The salt form most commonly sold is Hexarelin acetate. The compound is unambiguous regardless of label.
Cardiovascular biology and CD36 receptor pharmacology lead by volume — particularly ischemia-reperfusion injury models and cardioprotection signaling. Growth hormone axis research uses Hexarelin as a maximum-stimulation tool for diagnostic and pharmacological work. There's also active work in autophagy regulation and neuroprotection through ghrelin receptor signaling.
Yes — and the synergy is the basis for some diagnostic GH-stimulation tests. Hexarelin works through GHS-R1a; CJC-1295 and similar analogs work through GHRH receptors. Combining the two activates parallel pathways at the pituitary level, producing GH release larger than either compound alone. The hexarelin + GHRH combination has clinical pharmacology applications for testing pituitary reserve.
Native ghrelin is a 28-amino-acid peptide requiring octanoylation at serine-3 to be active. Hexarelin is a synthetic 6-amino-acid hexapeptide that doesn't need lipid modification to bind GHS-R1a. Hexarelin is also significantly more stable in circulation than ghrelin. The CD36 binding is an additional feature that ghrelin doesn't share at comparable potency, making Hexarelin a distinct pharmacological tool from its natural analog.
Researchers investigating ghrelin receptor pharmacology and growth hormone secretagogue potency consistently examine Hexarelin alongside compounds that span the full spectrum of GH-releasing activity. GHRP-2 and GHRP-6 are the direct hexapeptide comparators — all three are ghrelin mimetics with overlapping receptor profiles, but Hexarelin produces the strongest GH pulse of the three; researchers studying dose-response relationships and receptor desensitization in ghrelin mimetic pharmacology typically examine all three in parallel to map the potency spectrum. Ipamorelin represents the selectivity reference point — the weakest GH pulse in the ghrelin mimetic class but with the cleanest side effect profile, making it essential context for understanding what Hexarelin's additional potency costs in terms of cortisol and prolactin activation. Mod GRF (1-29) is the standard GHRH receptor pairing for Hexarelin in dual-receptor GH release research — combining the strongest available ghrelin mimetic with GHRH receptor activation produces the largest synergistic GH output in the secretagogue research toolkit. CJC-1295 DAC is sometimes examined alongside Hexarelin when researchers need to compare pulsatile high-amplitude GH release against sustained low-amplitude elevation — fundamentally different pharmacokinetic profiles for studying different aspects of GH axis biology.