Adipotide / FTPP 5mg
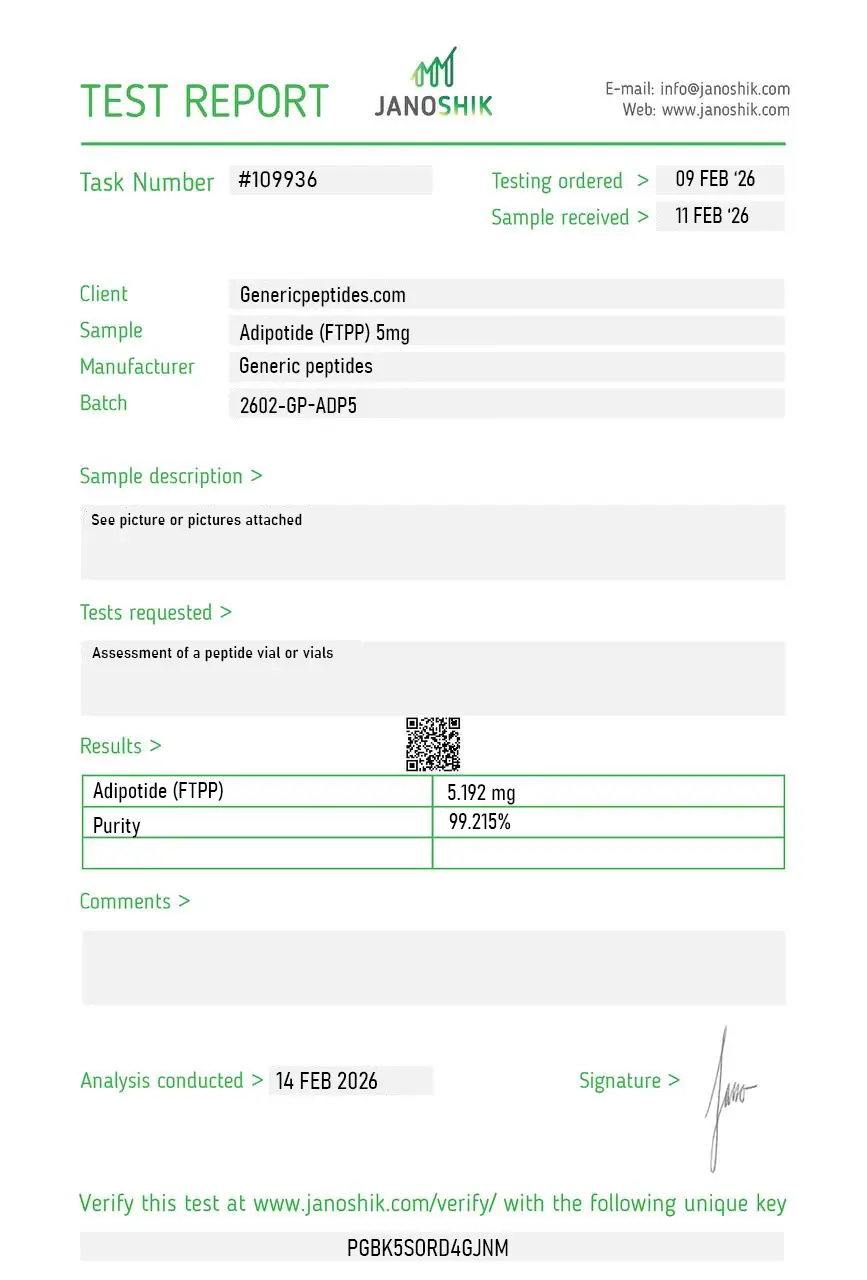
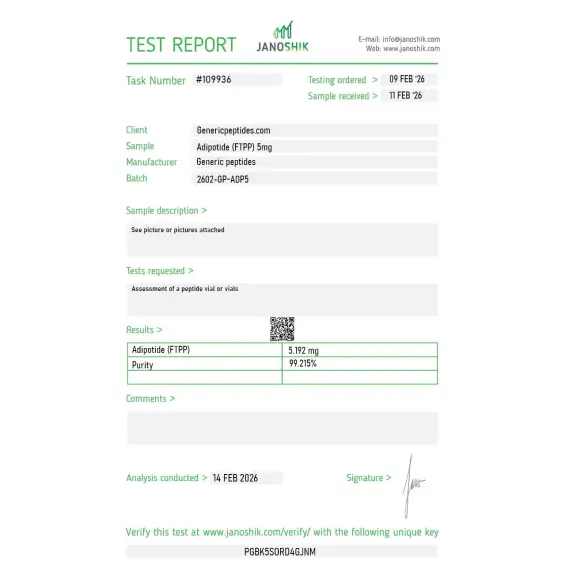
Certificate of Analysis available




Obese rhesus monkeys lost 11% of their body weight in 28 days. Not by suppressing appetite. Not by speeding up metabolism. By starving fat cells of their blood supply until they died. That's what Adipotide actually does — and that's why it's one of the most talked-about compounds in obesity research, even after clinical development paused.
Adipotide is a synthetic peptidomimetic — a peptide-like research compound — also called FTPP, which stands for Fat-Targeted Proapoptotic Peptide. It was developed at the MD Anderson Cancer Center to do something no other compound in this category does: kill the blood vessels that feed white fat tissue. Cut the supply line, and the fat cells starve. The compound has two parts working together — a homing sequence (CKGGRAKDC) that locks onto receptors found almost exclusively on fat-tissue blood vessels, and a proapoptotic payload that triggers cell death once it's bound. That's the mechanism in plain English.
Published in Science Translational Medicine in 2011 by Barnhart, Pasqualini, and colleagues. Spontaneously obese rhesus monkeys received Adipotide for 28 days. The treated animals lost between 7.4% and 14.7% of their body weight — averaging 11%. Imaging confirmed it was actual fat reduction, not water loss or muscle wasting. 38% reduction in total body fat. 27% reduction in abdominal fat. Insulin resistance improved at the same time. In rodent models, the response was even more dramatic — roughly 30% body weight reduction in obese mice. Most obesity drugs fail when they jump from rodents to primates. Adipotide didn't.
The animal data is extraordinary. The primate translation worked. And there's an uncomfortable truth that goes with it: the same 2011 study identified reversible kidney toxicity at the doses used. Elevated creatinine, structural changes in renal tubular cells. That finding is why human clinical development effectively stalled. Researchers studying Adipotide today work around that — lower exposures, different model systems, focused mechanistic questions. Anyone selling this as a guaranteed human fat-loss agent is ignoring the actual literature.
The honest position: Adipotide is one of the most mechanistically distinct compounds in the entire fat-metabolism research space. It's the only research peptide of its kind targeting prohibitin on fat vasculature directly. The science is real. The unanswered questions are real too — and that combination is exactly what makes it interesting for serious researchers.
Adipotide is a complex peptidomimetic — two functional domains joined by a linker, with a sequence (CKGGRAKDC-GG-D(KLAKLAK)₂) that's genuinely difficult to synthesize correctly. Cheap synthesis routes produce compromised products: incomplete sequences, wrong folding, missing the targeting domain entirely. For a compound where the entire point is selective binding to a specific receptor, sequence integrity isn't a nice-to-have. A poorly synthesized batch doesn't just give weaker results — it gives the wrong results.
Generic Peptides supplies research-grade Adipotide for sale at 99% purity, manufactured in the USA. Domestic synthesis, documented quality, and no guessing about whether the homing sequence in your vial is actually intact.
Order Adipotide (FTPP) for sale in the USA — 99% purity, full-sequence research grade.
It's a peptidomimetic — a peptide-like molecule built from a homing peptide sequence joined to a proapoptotic payload. So it's structurally peptide-based but functionally engineered, which is why you'll see it called both "peptide" and "research compound" in the literature. The accurate term is peptidomimetic.
Yes — Adipotide is legal to purchase in the United States for research purposes. It's not FDA-approved for human use, and clinical development was paused due to the kidney findings. As a research compound for laboratory use, it remains commercially available.
The 2011 primate study identified reversible kidney toxicity at therapeutic doses — elevated creatinine and renal tubular changes. That finding stalled clinical development. The mechanism still works. The therapeutic window for human use was the problem, not the underlying biology.
Completely different mechanisms. GLP-1 agonists work on appetite and insulin signaling — you eat less. Adipotide works on the blood vessels supplying fat tissue, so the fat cells lose their supply line and die. One controls intake. The other targets the tissue itself.
Yes. FTPP stands for Fat-Targeted Proapoptotic Peptide and it's the technical name. Adipotide is the name researchers used in the published primate study. Same compound, two labels — you'll see both in the literature.
Sources
Barnhart KF, Christianson DR et al. — "A Peptidomimetic Targeting White Fat Causes Weight Loss and Improved Insulin Resistance in Obese Monkeys." Science Translational Medicine, 2011. The MD Anderson primate study documenting 11% average weight loss and the kidney toxicity finding. https://pmc.ncbi.nlm.nih.gov/articles/PMC3666164/
Kolonin MG, Saha PK, Chan L, Pasqualini R, Arap W. — "Reversal of obesity by targeted ablation of adipose tissue." Nature Medicine, 2004. Original paper introducing the prohibitin-targeted vascular ablation concept and CKGGRAKDC homing peptide. https://pubmed.ncbi.nlm.nih.gov/15146197/
Science.org — Original publication of Barnhart et al. 2011 including the 7.4–14.7% weight-loss range and 38% body fat reduction figures. https://www.science.org/doi/10.1126/scitranslmed.3002621
ScienceDaily — MD Anderson Cancer Center press release on the primate study, supporting the mechanism description and 11% average weight-loss figure. https://www.sciencedaily.com/releases/2011/11/111109143009.htm
A compound this mechanistically specific demands sequence integrity. Generic Peptides delivers it.
Adipotide (FTPP) ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve the peptide's cyclic homing domain and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — protect from direct light and UV exposure to prevent photodegradation. | Keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Signs of Degradation | Healthy powder is white and loose. Watch for yellowing or darkening, clumping, visible moisture, or a sticky/damp texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
| Disulfide Bond Integrity | Adipotide contains a disulfide bond in its cyclic homing domain that's sensitive to reducing conditions and repeated freeze-thaw cycles. | Keep the vial sealed and stable; avoid temperature swings from frost-free freezers. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
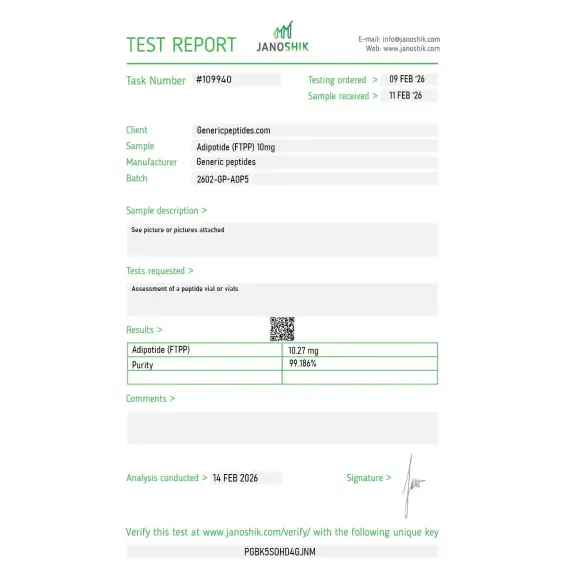
Independent lab test reports are available for Adipotide / FTPP 5mg and 10mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

We work on tumor-vasculature targeting and Adipotide is a useful reference for the homing-peptide-plus-proapoptotic-warhead architecture — the CKGGRAKDC motif fused to the KLAKLAK dimer. The targeting-domain-plus-effector-domain design is the actual research interest, independent of the adipose application it was named for. Material behaved as the construct should in our endothelial assays.
Reorder for the vascular-apoptosis line. Held up.
The KLAKLAK proapoptotic motif is the interesting part for us — it's a mitochondrial-membrane-disrupting D-peptide that's inert outside cells but lethal once internalized, which is why the homing domain matters for targeting. We study that conditional-lethality design. Adipotide is a clean example of the architecture and the material performed consistently.
Decent across two orders. The Arap and Pasqualini work at MD Anderson on vascular-homing peptides is the real foundation, and the listing could connect to that phage-display-derived targeting research rather than just naming the compound. It's a genuinely interesting body of work on tissue-specific vascular addresses. Compound itself was reliable.
Reconstituted clean. We handle it cautiously given it's a proapoptotic construct — single-use aliquots, careful concentration control, the discipline you'd apply to any cytotoxic tool compound. Ran consistently in our endothelial apoptosis assays. The targeted-destruction mechanism is the whole point and it delivered it in our model system.
Our reference for the homing-peptide-warhead construct class. Repeated orders, consistent. We study the vascular-targeting architecture; the compound's own clinical history ended on safety grounds, which is precisely the kind of context the popular framing of it omits.
The CKGGRAKDC homing sequence binds to prohibitin and annexin A2 receptors that are unusually concentrated on the blood vessels feeding white adipose tissue. Other tissues express these receptors at much lower levels, which gives Adipotide its selectivity. Once the homing peptide locks on, the proapoptotic payload triggers cell death in those specific blood vessels.
Tesofensine and most fat-loss compounds work centrally — they affect appetite, neurotransmitters, or metabolism through brain pathways. Adipotide does none of that. It physically destroys the blood supply to fat tissue without touching appetite signaling. That makes it mechanistically unique in the entire research category.
The targeting sequence is selective for white adipose tissue vasculature, with no apparent activity on brown fat. That selectivity is part of what makes it useful for studying the differences between fat types. Brown fat burns energy; white fat stores it — and Adipotide only attacks the storage type.
The compound has two functional domains joined by a linker, and synthesizing it correctly requires precise solid-phase peptide synthesis with proper purification. Suppliers cutting corners produce incomplete sequences or improperly folded products, which lose the targeting selectivity entirely. The result is a compound that looks like Adipotide on a label but doesn't bind correctly.
The 2011 primate study reported significant improvement in insulin resistance alongside the weight loss — and earlier mouse studies showed glucose tolerance improved within three days, before measurable fat loss occurred. That timing suggests the metabolic effects aren't purely a consequence of weight reduction.
The prohibitin-targeting concept was published by Kolonin and colleagues in 2004 in Nature Medicine, using rodent models of obesity. The primate study that made the compound widely known followed in 2011. The underlying research goes back nearly two decades at this point.
Adipotide isn't on the current WADA Prohibited List by name, though its mechanism could fall under broader anti-doping interpretation depending on how it's classified. It's not a common doping target because it's not commercially available as a pharmaceutical and has no oral bioavailability. Athletes should consult their governing body's specific rules.
Obesity and adipose tissue biology lead by far. There's also ongoing work in cancer research — the same prohibitin targeting concept extends to tumor vasculature in some contexts. Angiogenesis researchers use it as a tool to study selective vascular ablation.
Yes. Prohibitin-TP01 (Prohibitin-Targeting Peptide 1) is one of the technical names used in some scientific literature, referencing the receptor it binds. Adipotide and FTPP are the more common names. The full sequence — CKGGRAKDC-GG-D(KLAKLAK)₂ — is what identifies the molecule unambiguously.
Most peptidomimetics target enzymes or receptors to modify signaling. Adipotide is structural — it physically destroys the cells it binds to via mitochondrial disruption. That apoptosis-on-binding mechanism, combined with tissue-specific targeting, puts it in a category of its own among research peptides.