Somatropin 10 IU
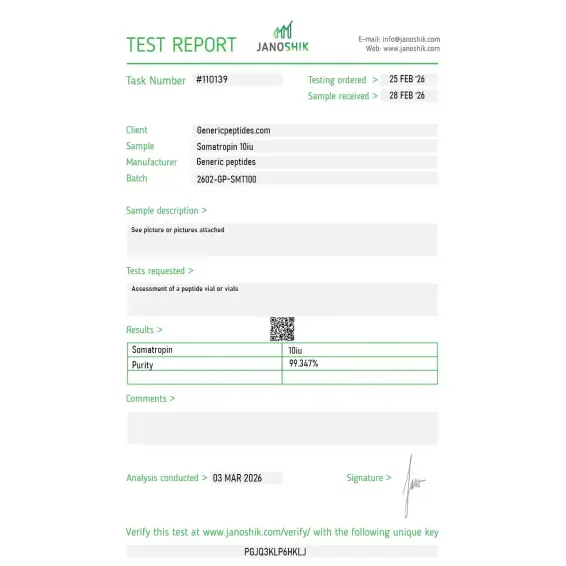
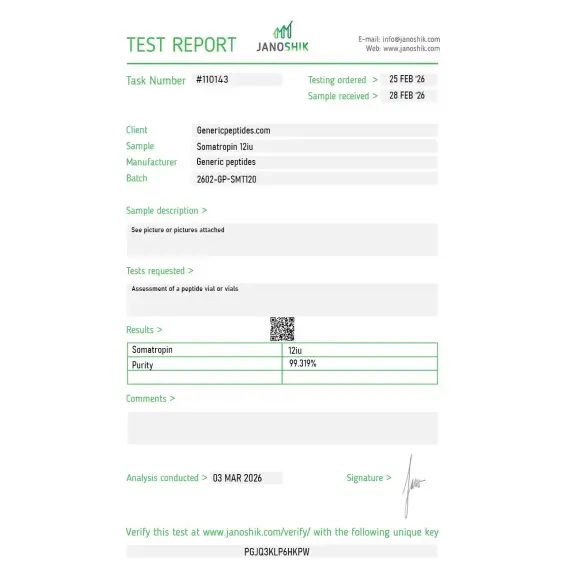
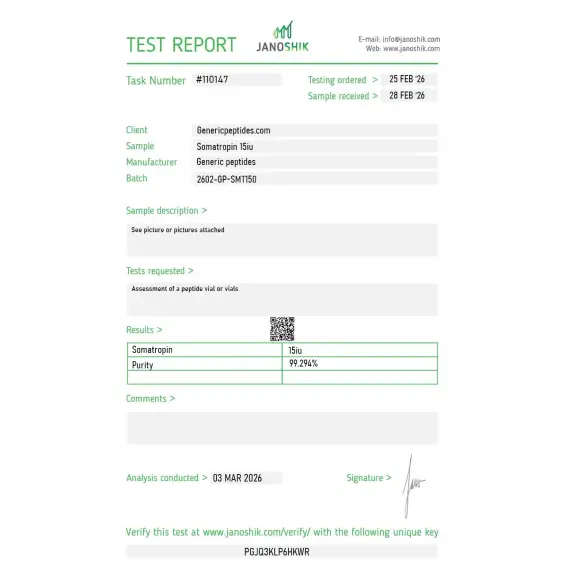
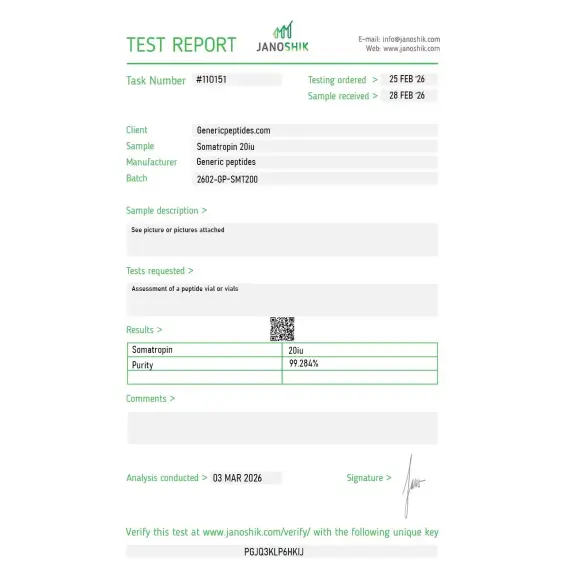
Certificate of Analysis available








Before 1985, the only human growth hormone available came from cadaver pituitary glands. Researchers extracted it after death, supply was severely limited, and a wave of Creutzfeldt-Jakob disease cases in the early 1980s — caused by prion contamination of cadaver-derived hormone — forced the FDA to discontinue its use entirely. Then Genentech did something extraordinary: they used recombinant DNA technology to manufacture a synthetic version identical to the natural hormone, sequence for sequence, in genetically modified bacteria. That recombinant compound is somatropin. Its 1985 FDA approval rewrote endocrinology.
Somatropin is recombinant human growth hormone (rhGH) — a 191-amino-acid protein with a molecular weight of approximately 22,125 daltons, manufactured to be chemically indistinguishable from the growth hormone naturally produced by the human pituitary gland. The recombinant production uses genetically modified Escherichia coli bacteria carrying a human GH gene plasmid, producing protein with the exact same amino acid sequence as endogenous human GH.
This is a fundamentally different category of compound from research peptides like BPC-157, GHRH analogs like Sermorelin, or growth hormone secretagogues like Ipamorelin. Those work indirectly — telling the pituitary to make and release more of its own GH. Somatropin is growth hormone, supplied directly. The mechanism bypasses the natural pituitary regulatory loops entirely. That's why it's both more powerful as a therapeutic tool and more pharmacologically blunt as a research probe.
GH binds to growth hormone receptors located on cell membranes throughout the body, but the most consequential binding happens in the liver. Hepatic GH receptor activation triggers production of insulin-like growth factors (IGF-1 and IGF-2) — the secondary messengers that produce most of GH's tissue-level effects. Linear growth, protein synthesis, lipolysis, and cellular proliferation all flow through the IGF-1 axis downstream of liver GH receptor activation.
The compound has eight FDA-approved indications across pediatric and adult medicine, including pediatric growth hormone deficiency, Turner syndrome, Noonan syndrome, Prader-Willi syndrome, SHOX deficiency, chronic renal insufficiency, idiopathic short stature, and small-for-gestational-age children with growth failure. Adult indications include adult-onset GH deficiency and HIV-associated wasting (Serostim). Eight different brand names are FDA-approved across the somatropin product family — Genotropin, Humatrope, Norditropin, Nutropin, Omnitrope, Saizen, Serostim, Zomacton — reflecting more than four decades of cumulative clinical development.
Here's the uncomfortable truth: somatropin has documented serious adverse event signals that other research peptides don't carry. The FDA has issued multiple safety communications regarding possible increased mortality risk, particularly in patients with chronic illness. Long-term overdosage produces gigantism or acromegaly. Carpal tunnel syndrome, fluid retention, insulin resistance, and intracranial hypertension occur at therapeutic doses. The compound's IGF-1-elevating effects also create theoretical concerns in cancer biology — IGF-1 signaling is implicated in proliferation in multiple tumor types. None of this means somatropin shouldn't be used; it means the pharmacology is consequential in ways that more selective research compounds aren't.
Sourcing matters more here than for almost any other product. The 191-amino-acid protein has a complex tertiary structure with two disulfide bonds essential for receptor binding. Recombinant production requires sophisticated cell culture systems, careful folding verification, and rigorous quality control. Counterfeit somatropin is a documented international black market problem — fake products, underdosed material, and contaminated preparations have been seized in athletic doping investigations across multiple countries.
Regulatory note: Somatropin is an FDA-approved prescription drug with extensive approved indications across pediatric and adult medicine. It is also a Schedule III controlled substance under US federal law — with a restriction unique among Schedule III substances: it is a federal crime to distribute or possess somatropin for any purpose other than treatment of a disease or condition recognized by the Secretary of Health and Human Services. This means somatropin occupies a categorically different legal position than other research peptides on this site. It requires a prescription for human use through approved channels. WADA prohibits somatropin for athletes in tested sports under category S2.2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics) — both in and out of competition.
Here's a sourcing problem that's specific to somatropin: it's a full-length 191-amino-acid recombinant protein with two essential disulfide bonds, not a synthesized peptide. Producing it correctly requires bacterial cell culture, proper protein folding, careful purification, and analytical verification of structural integrity. Cheap producers routinely deliver material with misfolded protein, scrambled disulfides, aggregated structures, or significant impurity content from incomplete purification. With a protein this complex, sequence-level analysis isn't enough — folding integrity determines whether the compound binds GH receptors at all. The international counterfeit market for HGH means even legitimate-looking labels often cover product that doesn't behave like real recombinant somatropin.
Generic Peptides supplies research-grade Somatropin for sale at 99% purity, manufactured in the USA. Domestic recombinant production with verified protein folding and disulfide structure — the part that determines whether your GH receptor binding assay produces published results or fails to replicate.
Order Somatropin for sale in the USA — 99% purity, full 191-amino-acid sequence with verified disulfide structure, manufactured domestically.
Somatropin is a Schedule III controlled substance with a unique federal restriction: it is a federal crime to distribute or possess it for any purpose other than treating a disease or condition recognized by the Secretary of HHS. This makes somatropin legally distinct from other research compounds on this site. FDA-approved brand names include Genotropin, Humatrope, Norditropin, Nutropin, Omnitrope, Saizen, Serostim, and Zomacton — all requiring a prescription for human use. WADA prohibits it for tested athletes.
Functionally yes, technically with one nuance. Somatropin is recombinant human growth hormone with a 191-amino-acid sequence identical to the natural hormone. "HGH" is sometimes used as a general term that can also refer to cadaver-derived GH (now banned), or to somatrem (an older recombinant version with one extra N-terminal amino acid). In modern medical usage, somatropin and HGH typically refer to the same recombinant 191-amino-acid product.
Direct vs indirect mechanism. Somatropin is growth hormone supplied externally — it bypasses the pituitary entirely. Sermorelin and other secretagogues stimulate the pituitary to release its own GH, preserving natural pulsatile patterns and feedback loops. Somatropin produces stronger GH levels but loses the natural regulatory architecture; secretagogues preserve regulation but produce more modest GH elevation.
Production complexity. Recombinant manufacturing of a 191-amino-acid protein with proper folding requires sophisticated cell culture systems, multi-step purification, and extensive analytical verification. Most research peptides are 5-30 amino acid synthetic chains made by automated solid-phase synthesis at much lower cost. The cost differential reflects fundamentally different manufacturing economics, not pure markup.
Almost certainly not the same product. The international counterfeit HGH market is well-documented in athletic doping investigations across multiple countries. Cheap online "somatropin" frequently turns out to be misfolded protein, underdosed material, contaminated preparations, or completely different compounds entirely. With recombinant proteins, label verification means almost nothing without extensive analytical confirmation.
Sources
FDA — "Somatropin Information." Official FDA page documenting eight pediatric indications, adult indications, and the safety communications regarding mortality risk. https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/somatropin-information
Omnitrope (somatropin) prescribing information. FDA-approved label documenting the 191-amino-acid recombinant DNA structure (E. coli production) and clinical pharmacology. https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/021426s043lbl.pdf
Richmond E, Rogol AD — "Treatment of Growth Hormone Deficiency in Children, Adolescents and at the Transitional Age." Documents the more than 50 years of GH treatment history, from cadaver pituitary GH (1958) to recombinant approval (1985). https://pmc.ncbi.nlm.nih.gov/articles/PMC3262362/
WADA — "Prohibited List" 2025. Documents Somatropin classification under category S2.2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics) for tested athletes. https://www.wada-ama.org/en/prohibited-list
191 amino acids. Two disulfide bonds. Folding determines whether the molecule works.
Somatropin (recombinant human growth hormone) ships as a sterile white lyophilized powder in a sealed vial or two-chamber cartridge, freeze-dried to preserve this 191-amino-acid protein and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition until the expiration date printed on the label. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Refrigerated at 2–8°C (36–46°F) until the printed expiration date, typically 18–36 months from manufacture. A few formulations (such as Serostim) are shipped stable at controlled room temperature — always check the product label. | Keep in the main body of the fridge, not the door, to avoid temperature swings. |
| Light Sensitivity | Yes — protect from direct light to prevent protein degradation. | Keep the vial in its original carton or box until ready to reconstitute. |
| Freezing | Not allowed. Freezing damages the protein's folded structure and permanently reduces potency for most somatropin formulations. | If a vial freezes accidentally, discard it — do not thaw and use. |
| Signs of Degradation | Healthy powder is white, dry, and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Storing in the fridge door where temperature fluctuates, placing near the freezer compartment, leaving out at room temperature, or keeping in a humid bathroom cabinet. | Keep it on a stable interior shelf in the fridge, and let it warm ~30 minutes at room temperature before use. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
Independent lab test reports are available for Somatropin 10 IU, 12 IU, 15 IU, and 20 IU batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.



Running low dose long term as part of a serious anti-aging protocol. IGF-1 levels tracking perfectly, sleep quality transformed, midsection responding better than any peptide stack I've run before. The difference between real Somatropin and underdosed product from cheap suppliers is enormous — quality matters more here than anywhere else. This supplier gets it right every single order.
Somatropin binds growth hormone receptors on cell membranes throughout the body, particularly in the liver. Hepatic GH receptor activation triggers production of insulin-like growth factors (IGF-1 and IGF-2), which mediate most of the downstream tissue-level effects — linear growth, protein synthesis, lipolysis, and cellular proliferation. The mechanism includes direct GH effects (lipolysis, glucose homeostasis) and indirect effects via the IGF-1 axis (somatic growth, anabolic processes).
Somatropin has the natural 191-amino-acid sequence identical to endogenous human GH. Somatrem (the older recombinant version) has one extra methionine residue at the N-terminus, making it 192 amino acids. Both have similar biological activity and potencies. Somatropin became the modern standard because the identical-to-natural sequence reduces immunogenicity concerns in chronic therapeutic use.
Before recombinant production, the only source of human GH was cadaver pituitary glands, which created severe supply limitations and contamination risks. The 1985 outbreak of Creutzfeldt-Jakob disease in cadaver-GH recipients led to FDA discontinuation of cadaver-derived GH entirely. Recombinant production using E. coli bacteria with human GH gene plasmids made unlimited, contamination-free synthesis possible.
Producing a 191-amino-acid recombinant protein with two essential disulfide bonds requires sophisticated cell culture systems, multi-step purification, and analytical verification of folding integrity. Cheap production routinely delivers misfolded protein, scrambled disulfides, or aggregated material that doesn't bind GH receptors properly. The international HGH counterfeit market complicates legitimate sourcing further — fake somatropin is a documented problem in athletic doping investigations.
Recombinant human growth hormone first received FDA approval for clinical treatment in 1985 — Genentech's Protropin (somatrem) was the original approval, followed by somatropin products. Indications have expanded over four decades to include eight pediatric conditions plus adult-onset GH deficiency and HIV-associated wasting. The compound has more than 40 years of clinical use history.
Yes. WADA prohibits Somatropin for athletes subject to drug testing under category S2.2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics) — both in and out of competition. The classification covers all forms of growth hormone including recombinant somatropin, somatrem, and analogs. Athletes in tested sports should avoid the compound regardless of how it's obtained.
The generic name is somatropin (INN). FDA-approved brand names include Genotropin, Humatrope, Nutropin, Nutropin AQ, Norditropin, Norditropin FlexPro, Omnitrope, Saizen, Serostim, and Zomacton. Generic descriptors include rhGH (recombinant human growth hormone), recombinant hGH, and somatotropin. CAS number 12629-01-5 for the 191-amino-acid recombinant protein.
Pediatric endocrinology and growth disorders lead historical clinical research volume. Aging-related GH decline studies, body composition research, sleep architecture (GH peaks during slow-wave sleep), and metabolic disease models are major research areas. There's also active work in HIV wasting (where Serostim is approved), critical illness (where GH was studied extensively then largely abandoned), and sports medicine doping research.
Direct upstream-downstream relationship. Somatropin binds liver GH receptors, triggering hepatic IGF-1 production. IGF-1 then mediates most of GH's tissue-level effects throughout the body — somatic growth, protein synthesis, anabolic metabolism. Some research peptides (IGF-1 LR3) supply IGF-1 directly; somatropin supplies GH, which then triggers natural IGF-1 production. Different research tools depending on which level of the GH/IGF-1 axis is the experimental target.
Mechanism and pharmacology. Somatropin <em>is</em> growth hormone, supplied directly — it bypasses pituitary regulation entirely and produces sustained GH elevation in circulation. GH secretagogues (Sermorelin, Ipamorelin, GHRPs) stimulate the pituitary to release its own GH, preserving pulsatile patterns and feedback regulation. Somatropin is more pharmacologically powerful but less physiologically natural. Different research tools for different mechanistic questions.
Researchers investigating the GH/IGF-1 axis, growth hormone replacement biology, and somatotropic signaling consistently examine Somatropin alongside compounds that target the same axis through indirect stimulation or downstream effector pathways. Sermorelin and Mod GRF (1-29) are the most natural secretagogue comparisons — both stimulate endogenous pituitary GH release rather than supplying exogenous hormone directly; researchers studying physiological pulsatile GH signaling vs pharmacological GH replacement examine all three to isolate the consequences of preserving vs bypassing natural pituitary regulation. Ipamorelin and GHRP-2 address the ghrelin receptor arm of the same pituitary axis — researchers studying comprehensive GH axis pharmacology examine ghrelin mimetics alongside direct GH replacement to map which regulatory pathway drives specific downstream outcomes. IGF-1 LR3 sits one step downstream — where Somatropin drives hepatic IGF-1 production indirectly, IGF-1 LR3 bypasses the liver entirely and activates IGF-1R directly; researchers studying the GH/IGF-1 axis often examine both to isolate hepatic vs peripheral contributions to anabolic and tissue-repair signaling. Tesamorelin is the only other GHRH-axis compound with FDA approval history — useful regulatory and pharmacological reference when researchers need to compare approved GH-axis interventions across different mechanism categories.