HCG 5K
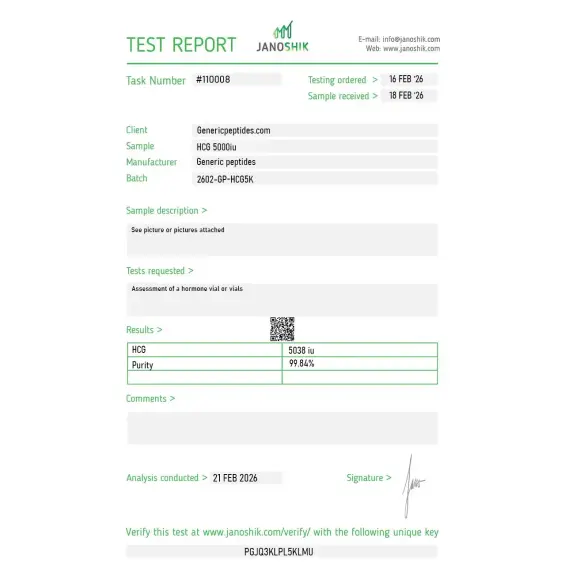
Certificate of Analysis available





HCG isn't a research peptide trying to find its place in clinical medicine. It's been an FDA-approved drug for decades — used in fertility clinics worldwide, prescribed alongside testosterone replacement to preserve fertility, and biochemically nearly identical to the body's own luteinizing hormone. The interesting story here isn't whether it works. It's why finding real, properly sourced HCG has gotten so difficult since 2020.
HCG (Human Chorionic Gonadotropin) is a glycoprotein hormone — not a synthetic research peptide, but a hormone naturally produced during pregnancy by the syncytiotrophoblast cells of the placenta. The medical product is either extracted from the urine of pregnant women (Pregnyl, Novarel) or produced via recombinant DNA technology (Ovidrel). It's structurally similar enough to luteinizing hormone (LH) that it binds the same receptor — the LH/CG receptor on Leydig cells in men and theca cells in women.
HCG is a heterodimer with alpha and beta subunits, each extensively glycosylated, with significant carbohydrate modifications that account for roughly a third of its total molecular mass. That receptor binding is the entire mechanism. In men, HCG tells the testes to produce testosterone and maintain sperm production. In women, it triggers ovulation. In children with undescended testicles (cryptorchidism), it can stimulate testicular descent. Three FDA-approved indications, all dating back decades.
On March 23, 2020, the Biologics Price Competition and Innovation Act took effect, reclassifying HCG from a drug to a biologic. That sounds technical. The practical impact was huge: compounding pharmacies — which had been a major supply source for HCG, especially for TRT-adjunct prescriptions — could no longer legally produce it without a Section 351 biologics license. Almost no compounding pharmacy has one. Supply effectively collapsed overnight.
Demand didn't collapse. It grew. TRT prescribing has surged in recent years, and HCG is the primary tool men use to preserve fertility while on testosterone. Add growing IVF demand and only three approved manufacturers (Organon for Pregnyl, Ferring for Novarel, EMD Serono for Ovidrel), and you get the chronic shortage that's persisted from 2020 through 2026. Cash prices that were $30-50 per vial pre-2020 are now $200-500. Patients regularly call multiple pharmacies to find any in stock.
HCG is not subject to the 503A bulks list process that governs research peptides — it was reclassified as a biologic under BPCIA in 2020, which is an entirely separate regulatory pathway. The compounding restriction has nothing to do with the recent BPC-157 / Epitalon / DSIP reclassification activity.
WADA prohibits HCG for male athletes in tested sports under category S2.3 (Chorionic Gonadotrophin and Luteinizing Hormone, prohibited in males). Female athletes are not subject to the same prohibition since HCG is endogenous to pregnancy. Athletes subject to drug testing should know this distinction.
For research applications: HCG remains commercially available as a research compound for laboratory work studying gonadotropin signaling, Leydig cell biology, ovarian reserve assessment, and reproductive endocrinology models. The compound is the same molecule whether it's labeled clinical or research grade — what differs is the supply chain and quality verification.
Here's a sourcing problem that's specific to HCG: it's a large, complex glycoprotein — not a simple peptide chain — and it's notoriously sensitive to handling, storage, and synthesis quality. Recombinant production requires sophisticated cell culture systems; urinary extraction requires careful purification. Either route is expensive when done correctly. Cheap HCG sourced from unverified manufacturers commonly arrives degraded, contaminated, or significantly underdosed. With a glycoprotein where biological activity depends on intact glycosylation patterns, "looks the same on the label" tells you nothing about whether the molecule still binds its receptor properly.
Generic Peptides supplies research-grade HCG for sale at 99% purity, manufactured in the USA. Domestic synthesis with verified glycoprotein integrity — the part that matters when you're studying receptor binding and the molecule's complex structure has to be intact.
Order HCG for sale in the USA — 99% purity, glycoprotein integrity verified, manufactured domestically.
Technically, no — HCG is a glycoprotein hormone, much larger and more complex than typical research peptides. It's a heterodimer with alpha and beta subunits, each glycosylated, with carbohydrate modifications accounting for a significant portion of its total mass. Research peptides are usually short amino acid chains; HCG is a full protein hormone with carbohydrate modifications that affect its biological activity.
HCG is FDA-approved as a prescription drug (Pregnyl, Novarel, Ovidrel) for three indications: female infertility, male hypogonadotropic hypogonadism, and pediatric cryptorchidism. As an FDA-approved biologic, it requires a prescription for human use. Sales as a research compound for laboratory use exist in a separate channel.
The 2020 FDA reclassification of HCG as a biologic eliminated most compounding pharmacy production almost overnight. Combined with only three approved manufacturers and growing demand from fertility clinics and TRT prescribing, this created a chronic shortage that's persisted through 2026. Cash prices increased dramatically as supply tightened.
They bind the same receptor and produce similar effects, but their pharmacokinetics differ dramatically. LH has a biological half-life of around 20 minutes; HCG has a half-life of 24-36 hours due to its glycosylation. That's why HCG is medically useful — you can't dose LH practically, but HCG provides sustained LH-like signaling from a single injection.
Probably not at the same purity or quality. Cheap online HCG often comes from unverified manufacturers where glycoprotein integrity isn't documented or controlled. Without verification, you're trusting a label on a complex biologic that requires sophisticated production to make correctly. The price gap reflects manufacturing quality, not pure markup.
Sources
FDA — Pregnyl prescribing information and approved indications. Documents the FDA-approved status, mechanism, and indications for HCG. https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/017016s039lbl.pdf
Rainer Q et al. — "The Safety of Human Chorionic Gonadotropin Monotherapy Among Men With Previous Exogenous Testosterone Use." Cureus, 2022. Documents HCG's role as alternative to TRT and AUA guideline support. https://pmc.ncbi.nlm.nih.gov/articles/PMC9271319/
The availability of gonadotropin therapy from FDA-approved pharmacies for men with hypogonadism and infertility. PMC, 2023. Documents the post-2020 supply collapse and 503B compounding pharmacy survey. https://pmc.ncbi.nlm.nih.gov/articles/PMC10083688/
WADA — Prohibited List 2025. Documents HCG classification under category S2.3 (Chorionic Gonadotrophin) for male athletes. https://www.wada-ama.org/en/prohibited-list
Glycoprotein integrity isn't optional — it's the entire molecule. 99% purity, USA-made, structure verified.
HCG (Human Chorionic Gonadotropin) ships as a sterile white lyophilized powder in a sealed glass vial, freeze-dried to preserve the glycoprotein hormone and extend its shelf life. With a few simple habits — cool, dark, dry — the sealed vial stays in perfect condition until the expiration date printed on the label. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Controlled room temperature at 15–30°C (59–86°F) until the printed expiration date, typically 18–24 months from manufacture. Refrigeration at 2–8°C (36–46°F) is also acceptable and may extend usable life. | A cool, dark cabinet works for most labels; a fridge is fine if your room is often warm. |
| Light Sensitivity | Yes — protect from direct light to prevent hormone degradation. | Keep in the original box or carton until ready to reconstitute. |
| Freezing | Allowed for the unreconstituted powder only. Freezing at or below −15°C (5°F) can preserve potency for up to several years. Never freeze the reconstituted solution — it damages the glycoprotein structure. | Freeze only if you're storing beyond the printed expiration date. |
| Signs of Degradation | Healthy powder is white, dry, and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Storing near a heat source (stove, radiator, sunny windowsill), keeping in a humid bathroom cabinet, or opening a cold vial and letting condensation form inside. | Keep in a cool, dark spot, and let refrigerated or frozen vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
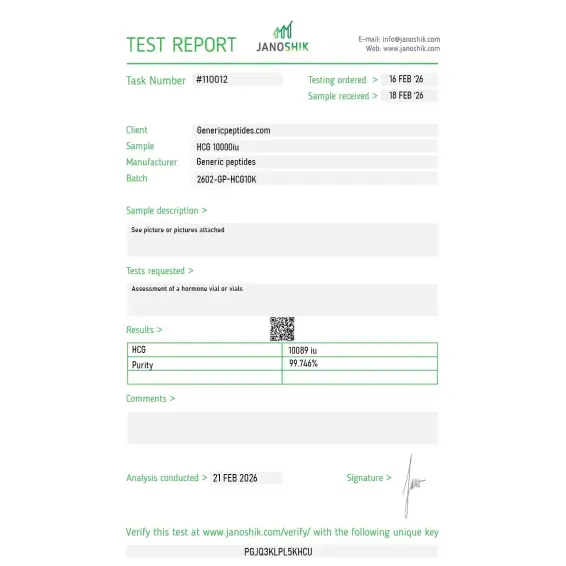
Independent lab test reports are available for HCG 5K and 10K batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

LH/CG receptor activation in transfected cell lines — needed the urinary-derived preparation to match our reference protocols, since the recombinant gives a cleaner glycoform but a slightly different activation profile. The product page disclosed the source explicitly. Consistent across the conditions we ran.
The thing to confirm before ordering is whether it's urinary-derived or recombinant — the source determines the glycoform profile, and protocols built on one don't necessarily transfer to the other. This vendor disclosed it. Star off because for a heterodimeric glycoprotein the COA should report more than HPLC purity — the α and β subunit integrity and the glycoform aren't captured by a single purity number.
We use it for Leydig cell stimulation assays — characterizing testosterone-biosynthesis kinetics in primary culture, with HCG as the LH-receptor agonist driving the response. The 5000-IU vial format suited our dilution series across plates. Bioactivity held across the working period. Reconstituted in the supplied buffer, aliquoted, stored cold.
We pair HCG with HMG in reproductive-biology research — HMG for follicular development, HCG for the ovulation trigger, the classic two-step protocol. Sourcing both from one catalog with matched documentation keeps the procurement clean and the records consistent. That sequential pairing is the experimental design.
What I value is the source transparency — urinary-derived stated upfront rather than left ambiguous. For a glycoprotein where the production source shifts the glycoform and the receptor-activation kinetics, knowing which preparation you're getting before ordering saves a clarification email and a potential protocol mismatch. Material consistent.
For LH-receptor pharmacology we run HCG against recombinant LH side by side — HCG has the longer half-life through its C-terminal extension on the β subunit, so the activation kinetics differ even though they hit the same receptor. Sourcing the comparison material consistently matters. That half-life contrast at the shared receptor is the experiment.
The structural feature that makes HCG distinct from LH is the C-terminal peptide extension on the β subunit — it's what gives the roughly sixfold longer half-life at the shared LH/CG receptor. For studying sustained receptor activation versus the shorter LH pulse, that extended-half-life property is exactly the tool. Material behaved as the receptor pharmacology predicts.
We work the veterinary research angle — synchronized ovulation in a research-animal model, where HCG's LH-like activity triggers the ovulatory response. The IU activity was consistent with the protocol requirement and the lyophilized preparation survived domestic shipping intact against our internal reference. Cold pack included on that order, which matters for the glycoprotein.
HCG binds to the LH/CG receptor on Leydig cells in men and theca cells in women — the same receptor that luteinizing hormone (LH) uses. In men, this triggers testosterone production directly inside the testes. In women, it can trigger ovulation when given at the right point in the menstrual cycle. The mechanism is essentially hormone receptor activation, not the indirect signaling cascades that most peptides use.
Pregnyl (Organon) and Novarel (Ferring) are urinary-derived HCG — extracted from the urine of pregnant women and purified. Ovidrel (EMD Serono) is recombinant HCG made via DNA technology. The recombinant version comes pre-filled in a syringe at 250 mcg, while urinary versions come as 10,000 IU vials requiring reconstitution. Functionally similar; structurally and pharmacokinetically slightly different.
The mechanism supports it, and clinical evidence is reasonable. Up to 60% of men on exogenous testosterone develop azoospermia (zero sperm) due to suppressed pituitary signaling. HCG bypasses the pituitary suppression by directly stimulating Leydig cells to maintain intratesticular testosterone — which is required for spermatogenesis. The American Urological Association recommends it for testosterone-deficient men who want to preserve fertility.
HCG is a glycoprotein hormone with complex tertiary structure and glycosylation patterns that determine biological activity. Production requires either careful urinary extraction with multi-step purification or recombinant cell culture with proper folding. Cheap manufacturing routinely produces material with damaged glycosylation, aggregated protein, or significant impurity profiles that affect receptor binding without changing how it looks on a label.
HCG has been in clinical use since the 1930s, originally for ovulation induction and later expanded to male infertility and cryptorchidism applications. It was one of the first hormones successfully used as a therapeutic agent. The FDA approval framework dates back to before the modern regulatory system was established — HCG was grandfathered into approved status.
For male athletes, yes. WADA prohibits chorionic gonadotrophin and luteinizing hormone (and their releasing factors) for males under category S2.3 — both in and out of competition. Female athletes aren't subject to the same prohibition since HCG is naturally produced during pregnancy. Male athletes subject to drug testing should avoid HCG regardless of indication.
Substantial. The "HCG diet" used homeopathic dilutions or oral drops that the FDA banned in 2011 as fraudulent. Real prescription HCG is an injectable biologic; the homeopathic versions contained no functional HCG at all. The diet protocol itself (500-calorie diet) was the only thing producing weight loss — the "HCG" component was inactive.
Human Chorionic Gonadotropin, Chorionic Gonadotropin, Chorionic Gonadotrophin (British spelling), and the brand names Pregnyl, Novarel, and Ovidrel. Generic versions exist from select manufacturers. The molecule is the same across these names — what varies is the source (urinary vs recombinant) and the salt formulation.
Reproductive endocrinology leads by volume — Leydig cell biology, ovarian function, and gonadotropin receptor signaling. There's also active work in pregnancy biology, placental function, and HCG's role as a possible immunomodulator (some research has explored its role in transplant rejection prevention). Cancer research has investigated ectopic HCG production by certain tumors.
What makes HCG different from other gonadotropins like FSH?
Researchers investigating reproductive endocrinology, gonadotropin signaling, and hormonal axis regulation consistently examine HCG alongside compounds that target overlapping or complementary reproductive pathways. HMG (Human Menopausal Gonadotropin) is the most natural pairing — HCG provides LH-equivalent activity while HMG provides both FSH and LH activity; researchers studying follicular development, ovarian stimulation, and male fertility protocols typically examine both to isolate the contributions of each gonadotropin component. Kisspeptin-10 sits upstream of the entire HPG axis — activating GnRH release which then drives LH and FSH secretion — making it a useful research tool for studying the regulatory signals that govern gonadotropin production rather than the gonadotropins themselves. Sermorelin and Tesamorelin occasionally appear in the same research context when studying hormonal interactions between the GH axis and reproductive axis, particularly in male hypogonadism and body composition research where both axes are dysregulated simultaneously. Each represents a different point of entry into the same hypothalamic-pituitary-gonadal biology that HCG research addresses.