Tesamorelin 2mg
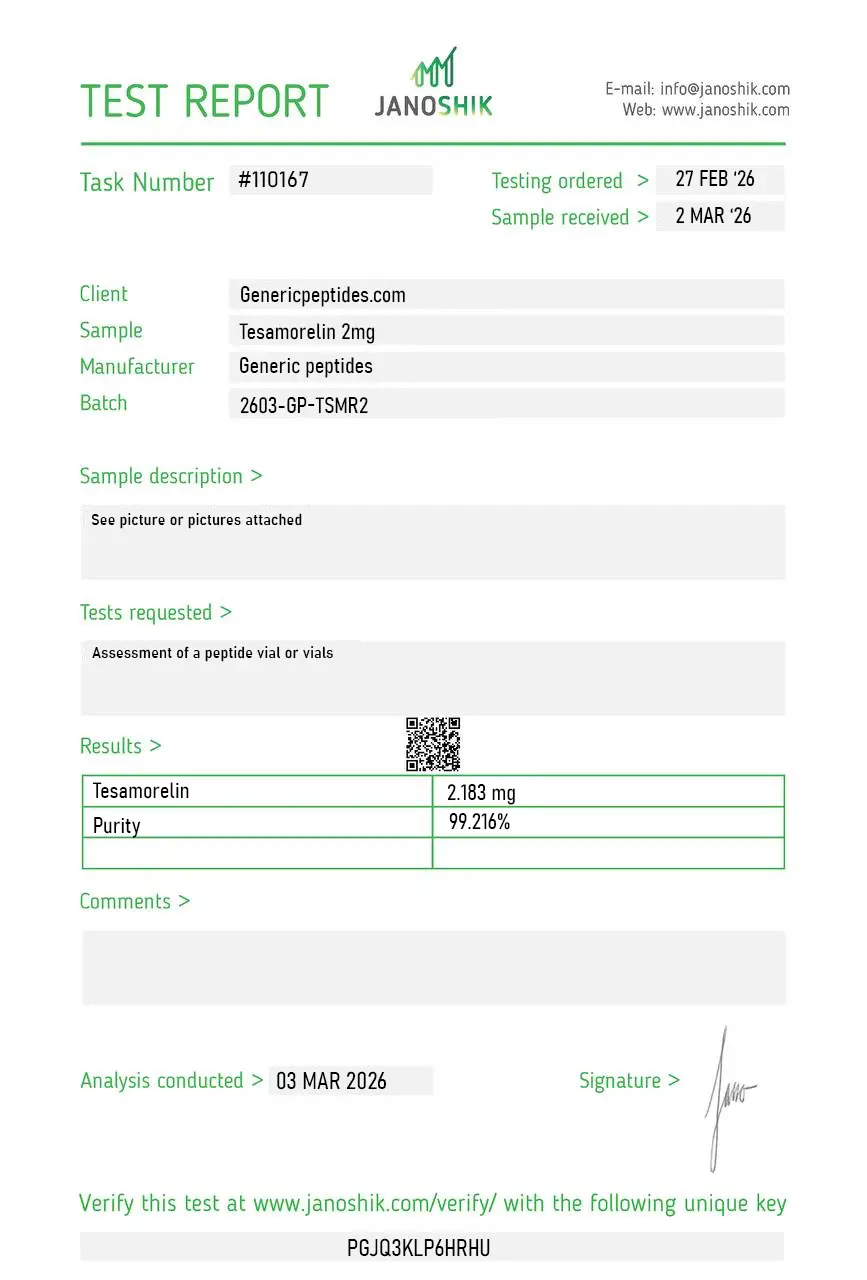
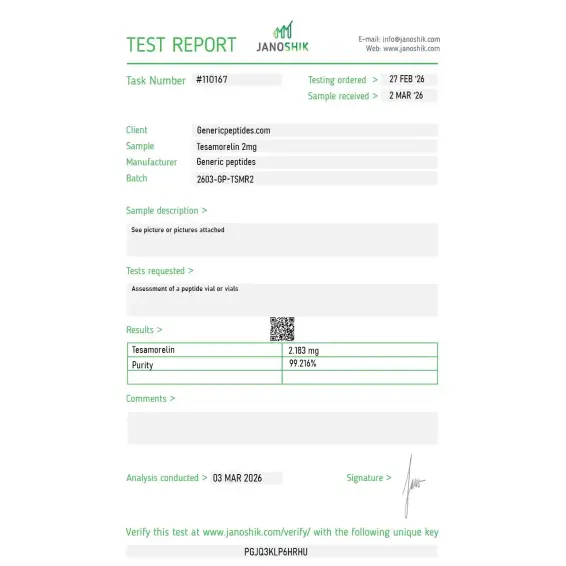
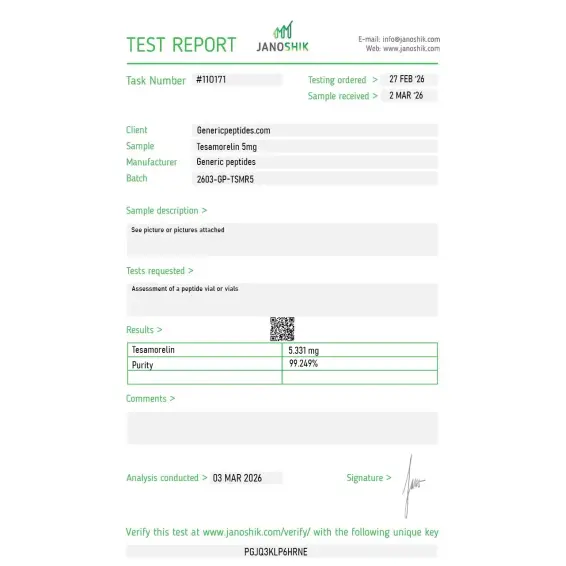
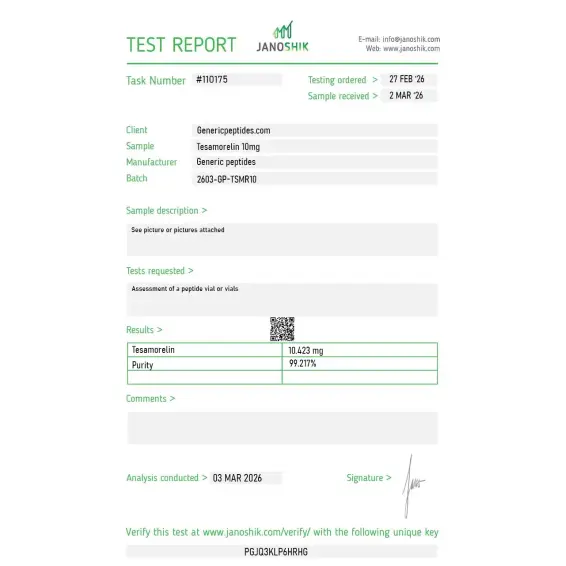
Certificate of Analysis available







Most GHRH analogs in the research peptide market never made it through clinical trials. Tesamorelin did. The FDA approved it in November 2010 as the only medication ever specifically indicated for one of the strangest side effects of antiretroviral therapy: visceral fat accumulation in HIV patients. The compound has stayed approved continuously for fifteen years, with a new improved formulation (EGRIFTA WR) approved in March 2025. That's longer than nearly any GHRH analog has stayed on the market — and it's exactly why Tesamorelin's research base is fundamentally different from research-only GHRH peptides.
Tesamorelin is a synthetic 44-amino-acid analog of natural human GHRH (growth hormone-releasing hormone). It uses the full GHRH 1-44 sequence — not the 29-amino-acid truncated version that Sermorelin, CJC-1295, and Mod GRF 1-29 are based on. The pharmacological enhancement is a single chemical modification: a trans-3-hexenoic acid group bonded to the N-terminal tyrosine residue. That fatty acid attachment doesn't change the amino acid sequence — it adds a small lipophilic group that resists enzymatic degradation by dipeptidyl peptidase-4 and extends half-life beyond what unmodified GHRH achieves.
What that engineering produces: a GHRH analog with biological activity essentially identical to natural GHRH at the receptor level, but with a half-life extended enough for once-daily clinical dosing. The mechanism is physiological — Tesamorelin stimulates the anterior pituitary to make and release its own growth hormone in natural pulsatile patterns, preserving the negative feedback loops that regulate the somatotropic axis. It doesn't supply GH directly the way somatropin does. It restores the natural signal.
The clinical story behind Tesamorelin's FDA approval is unusual. HIV patients on antiretroviral therapy frequently develop HIV-associated lipodystrophy — characterized by abdominal fat accumulation alongside subcutaneous fat loss in the face and limbs, plus metabolic complications. The condition is disfiguring and metabolically harmful, and patients with HIV-associated lipodystrophy generally show decreased growth hormone secretion. That GH deficiency contributes directly to the visceral fat accumulation, since GH normally drives lipolysis in adipose tissue.
Tesamorelin restores GH/IGF-1 axis function, which in turn drives visceral fat reduction without requiring the pharmacological GH excess that direct somatropin produces. The Phase 3 trials that supported FDA approval demonstrated significant reduction in visceral adipose tissue (VAT) over 26 weeks, with effects sustained over 52 weeks of continued treatment. The 2014 Stanley publications extended the work into liver fat reduction in HIV patients with hepatic steatosis. More recent NIH-supported research has investigated cognitive function effects in aging adults, NAFLD/NASH applications, and broader metabolic biology.
Here's the honest part: Tesamorelin's FDA-approved indication is narrow. It's specifically for HIV-associated lipodystrophy. Off-label use has expanded into general body composition optimization, NAFLD, cognitive aging, and metabolic disease, but those applications don't have the same regulatory backing. The cardiovascular safety profile is reassuring — the 2017 Falutz long-term safety analysis didn't find significant cardiovascular signals. Common adverse events include injection site reactions, joint pain, and peripheral edema. Less common but more serious concerns include glucose intolerance and the theoretical IGF-1 elevation issues that any GH-axis stimulator carries.
Sourcing matters here in ways that don't apply to most peptides. Tesamorelin's regulatory history includes actual FDA-approved products with documented manufacturing standards. Compounded and research-grade versions exist in a gray space where quality control varies dramatically. With the brand-name product priced at over $2,000 monthly, the economic incentive to substitute lower-quality material is substantial.
Regulatory note: Tesamorelin is an FDA-approved prescription drug (EGRIFTA, EGRIFTA SV, EGRIFTA WR — all from Theratechnologies). The approval is for HIV-associated lipodystrophy specifically. It's not on the 503A bulks list because it's a fully approved drug — different regulatory category from peptides currently in compounding-status transition. Notably, in 2020 Tesamorelin was reclassified as a biologic alongside HCG under the BPCIA — removing traditional 503A/503B compounding exemptions. As with HCG, a biologics license would be required to compound it, which virtually no compounding pharmacy holds. WADA prohibits Tesamorelin for athletes in tested sports under category S2 (Peptide Hormones, Growth Factors, Related Substances). Sales as a research compound for laboratory use continue legally in a separate channel.
Here's a sourcing problem that's specific to Tesamorelin: the trans-3-hexenoic acid modification at the N-terminal tyrosine is the entire reason this compound exists as a distinct pharmaceutical. Without that modification, you have natural GHRH (or something like Sermorelin) — which has a half-life of minutes rather than hours and a completely different research profile. Cheap synthesis routes routinely deliver under-modified material, fatty acid attached at the wrong position, or unmodified GHRH 1-44 mislabeled as Tesamorelin. The 44-amino-acid backbone alone isn't Tesamorelin — the modification is what makes it pharmacologically distinct. Without HPLC-MS verification specifically targeting the N-terminal modification, the difference between real Tesamorelin and mislabeled GHRH is invisible to buyers but ruins any pharmacokinetic study trying to replicate published data.
Generic Peptides supplies research-grade Tesamorelin for sale at 99% purity, manufactured in the USA. Domestic synthesis with verified trans-3-hexenoic acid modification — the part that determines whether you have actual Tesamorelin or accidentally-purchased-natural-GHRH pharmacokinetics.
Order Tesamorelin for sale in the USA — 99% purity, verified N-terminal modification, manufactured domestically.
Yes — Tesamorelin is legally available for laboratory research use in the United States. As an FDA-approved prescription drug under the brand names EGRIFTA, EGRIFTA SV, and EGRIFTA WR (Theratechnologies), it requires a prescription for human use through approved channels. Sales as a research compound for laboratory work exist in a separate regulatory channel. WADA prohibits it for tested athletes.
Different sequences and different stability strategies. Tesamorelin uses the full natural 44-amino-acid GHRH sequence with a trans-3-hexenoic acid modification at the N-terminus. Sermorelin uses only the first 29 amino acids of GHRH (the active fragment) with no modifications. Tesamorelin has a longer half-life and is FDA-approved for HIV lipodystrophy specifically; Sermorelin was originally FDA-approved for pediatric GH deficiency.
Both are stability-enhanced GHRH analogs but with different engineering approaches. CJC-1295 uses the 29-amino-acid GHRH backbone with four amino acid substitutions to resist enzymatic cleavage. Tesamorelin uses the full 44-amino-acid sequence with a fatty acid N-terminal modification. Tesamorelin has FDA approval; CJC-1295 doesn't. Different research tools with different regulatory pathways.
HIV patients on antiretroviral therapy frequently develop visceral adiposity alongside reduced GH secretion — a metabolic syndrome where Tesamorelin's GH-axis restoration directly addresses the underlying mechanism. The Phase 3 trials demonstrated significant visceral fat reduction in this specific population. Other obesity types weren't part of the approval pathway, though research has expanded into broader applications.
Probably not. The trans-3-hexenoic acid modification is the technically demanding, expensive part of Tesamorelin synthesis. Cheap producers routinely deliver under-modified material or unmodified GHRH 1-44 mislabeled as Tesamorelin. Without HPLC-MS verification of the N-terminal modification, the difference is invisible until your half-life data doesn't match published research. The pharmacokinetic profile that defines this compound's research utility may not actually be there.
Sources
EGRIFTA prescribing information. FDA-approved label documenting the 44-amino-acid GHRH structure with trans-3-hexenoic acid modification, mechanism of action, and HIV-associated lipodystrophy indication. https://www.accessdata.fda.gov/drugsatfda_docs/label/2013/022505s004lbl.pdf
Falutz J et al. — "Effects of tesamorelin (TH9507), a growth hormone-releasing factor analog, in human immunodeficiency virus-infected patients with excess abdominal fat: a pooled analysis of two multicenter, double-blind placebo-controlled phase 3 trials." JCEM, 2010. The pivotal Phase 3 efficacy data. https://pubmed.ncbi.nlm.nih.gov/20660034/
Stanley TL, Feldpausch MN, Oh J et al. — "Effect of tesamorelin on visceral fat and liver fat in HIV-infected patients with abdominal fat accumulation: a randomized clinical trial." JAMA, 2014. Documents liver fat reduction in HIV patients. https://pubmed.ncbi.nlm.nih.gov/25244183/
Theratechnologies — "FDA Approval of EGRIFTA WR (Tesamorelin F8)," March 25, 2025. Documents the new FDA-approved formulation with weekly reconstitution. https://www.theratech.com/news-releases/news-release-details/theratechnologies-receives-fda-approval-egrifta-wrtm-tesamorelin/
FDA-approved GHRH analog. The N-terminal modification is what makes it different from everything else.
Tesamorelin ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve its 44-amino-acid modified GHRH structure and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — protect from direct light and UV exposure to prevent photodegradation. | Keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | Tesamorelin contains a methionine residue that's prone to oxidation if the vial seal is broken or the powder is exposed to air. | Keep the aluminum crimp cap intact until ready to reconstitute. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
Independent lab test reports are available for Tesamorelin 2mg, 5mg, and 10mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.


The reason to choose this over sermorelin or the GRF(1-29) fragments is that it's the full 44-residue sequence with the N-terminal hexenoyl modification — closest thing to native GHRH with extended stability. Most catalogs lump all the GHRH analogs together as interchangeable. They aren't. Material activated the receptor consistently. Star off because the trans-3-hexenoic acid isomer wasn't explicitly confirmed and for this compound the specific isomer matters.
Among the GHRH analogs this is one of only two with an actual FDA approval behind it — Egrifta, for HIV lipodystrophy. That clinical validation makes it a more defensible reference compound for receptor work than the never-approved analogs. The listing acknowledges the Theratechnologies development heritage, which I appreciate.
What's distinctive about this compound pharmacologically is the visceral-versus-subcutaneous fat selectivity — the Phase 3 data showed it preferentially hits VAT. For our adipose-depot differential work that selectivity is the entire reason we use it rather than a generic GH secretagogue. Material held up across the dose range we tested.
Reorder. Adipocyte depot studies. The lipidated peptide handling is consistent batch to batch.
The hexenoyl lipidation gives this slightly different solubility behavior than the unmodified GRF fragments — the lipid moiety adds a bit of hydrophobic character but it stays workable in aqueous buffer at our concentrations. Took one trial run to dial in the handling. Nothing problematic, just different from the truncated analogs.
Theratechnologies' clinical data on this is genuinely substantial — the Phase 3 VAT-reduction numbers, the SV reformulation, decades of development. The listing treats it as the characterized pharmaceutical it is rather than a generic "fat-loss peptide," which is the framing it deserves and rarely gets.
GHRH receptor activation, full-length analog. cAMP response as expected.
Tesamorelin binds GHRH receptors on pituitary somatotrophs, stimulating endogenous growth hormone release in natural pulsatile patterns. The increased GH activates lipolysis directly in visceral adipose tissue and indirectly through IGF-1 elevation. The mechanism is physiological — restoring GH-axis function rather than producing pharmacological GH excess. In HIV patients with reduced GH secretion, this restoration specifically targets the underlying metabolic deficiency.
Mechanism and pharmacology. Direct HGH (somatropin) supplies growth hormone exogenously, bypassing the pituitary entirely and producing sustained supraphysiological GH levels. Tesamorelin stimulates the pituitary to release its own GH in natural pulsatile patterns, preserving feedback regulation. Tesamorelin produces more modest effects with better physiological integration; HGH produces stronger effects with broader off-target consequences.
HIV patients on antiretroviral therapy commonly develop visceral fat accumulation alongside reduced growth hormone secretion. The metabolic dysfunction is partly mediated by this GH deficiency. Tesamorelin restores GH-axis function in this specific population, which directly addresses the underlying mechanism of visceral adiposity. The targeted approach is what supported FDA approval for this indication specifically.
The trans-3-hexenoic acid modification at the N-terminal tyrosine is the technically demanding, expensive part of synthesis. Cheap producers routinely deliver under-modified material, fatty acid attached at the wrong position, or unmodified GHRH 1-44 mislabeled as Tesamorelin. Detection requires HPLC-MS analysis specifically targeting the N-terminal modification — most budget suppliers don't run this verification.
Tesamorelin was developed by Theratechnologies (originally as TH9507), a Montreal-based biopharmaceutical company. The Phase 3 trials supporting FDA approval were conducted in the late 2000s. FDA approval came in November 2010 as EGRIFTA. Subsequent formulations include EGRIFTA SV (improved reconstitution) and EGRIFTA WR (March 2025, weekly reconstitution with smaller injection volume).
Yes. WADA prohibits Tesamorelin for athletes subject to drug testing under category S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). All GHRH analogs are covered under this classification. Athletes in tested sports should avoid the compound regardless of its FDA-approved status for HIV lipodystrophy.
Tesamorelin acetate (the salt form), TH9507 (the original development code from Theratechnologies), and brand names EGRIFTA, EGRIFTA SV, and EGRIFTA WR. Generic descriptors include GHRH (1-44) trans-3-hexenoyl analog. CAS number 218949-48-5 (free base). Different naming conventions across literature, all referring to the same modified 44-amino-acid peptide.
HIV-associated lipodystrophy and visceral adiposity research lead by clinical volume. Beyond the FDA-approved indication, active research includes nonalcoholic fatty liver disease (NAFLD/NASH) — particularly the Stanley group's work at Massachusetts General Hospital, cognitive function in aging adults (NIH-supported studies), insulin resistance, and general metabolic health. The compound serves as a model GHRH analog in pituitary function research.
No. In 2020, Tesamorelin was reclassified as a biologic alongside HCG, which removed traditional compounding pharmacy production pathways. The reclassification was part of the broader BPCIA regulatory framework affecting biologic vs drug status. As an FDA-approved biologic, Tesamorelin is available only through approved channels for human use, with limited research compound availability for laboratory work in a separate regulatory channel.
Sequence-wise, almost nothing — Tesamorelin uses the full natural 44-amino-acid GHRH sequence. The difference is the trans-3-hexenoic acid modification at the N-terminal tyrosine, which provides resistance to enzymatic degradation and extended pharmacokinetics. Native GHRH has a 7-minute half-life; Tesamorelin's modification extends this enough for once-daily clinical dosing while preserving full GHRH receptor binding and biological activity.
Researchers investigating GHRH analog pharmacology, GH/IGF-1 axis biology, and metabolic applications of growth hormone restoration consistently examine Tesamorelin alongside compounds that target overlapping or complementary aspects of GH axis and fat metabolism research. Sermorelin is the most natural regulatory and structural comparison — both are the only GHRH analogs with prior FDA approval history, both stimulate physiological pulsatile GH release, and researchers studying the pharmacological contribution of different GHRH sequence lengths and stability modifications examine both to isolate how the full 44-amino-acid sequence vs the truncated 29-amino-acid sequence affects receptor binding and downstream GH output. Mod GRF (1-29) represents the research-compound end of the GHRH analog spectrum — same 29-amino-acid active fragment with four stability substitutions but without FDA approval history, useful when researchers need a shorter-acting GHRH reference with well-characterized receptor pharmacology. Ipamorelin and CJC-1295 DAC address the ghrelin receptor arm of the same pituitary axis — researchers studying comprehensive dual-receptor GH stimulation sometimes examine ghrelin mimetics alongside Tesamorelin to compare GHRH-only vs combined receptor activation. Semaglutide and Tirzepatide occasionally appear in the same metabolic research context given Tesamorelin's visceral fat reduction mechanism — researchers studying different pharmacological approaches to visceral adiposity sometimes examine GLP-1/GIP receptor agonists alongside GHRH-mediated GH restoration to compare appetite-driven vs GH axis-driven fat metabolism effects.