Glutathione 200mg
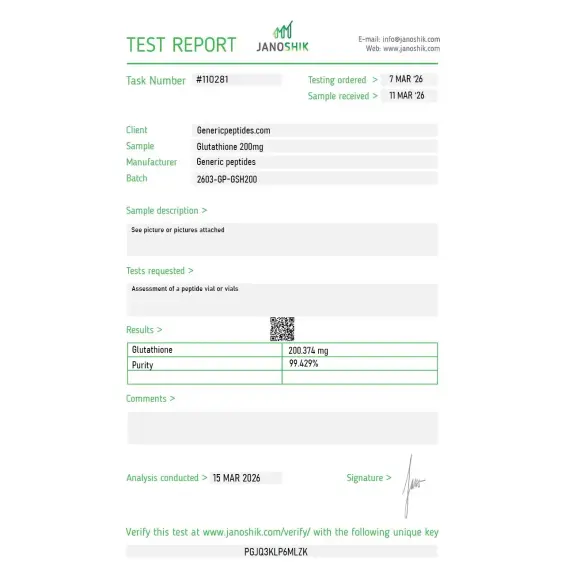
Certificate of Analysis available




French chemist De-Rey Pailhade discovered glutathione in 1888 — three years before the peptide bond had even been formally proposed in chemistry. He found it in blood, sheep brain, fish, and vegetables. He named it "philothion" (Greek for "loving sulfur") because of its strong reactivity with sulfur compounds. Hopkins renamed it glutathione 33 years later. Inside every cell in your body, this tripeptide reaches concentrations as high as 15 millimolar — making it more abundant than nearly any other intracellular molecule outside of basic structural proteins.
Glutathione (GSH) is a tripeptide with the sequence γ-glutamyl-cysteinyl-glycine — three amino acids joined by an unusual γ-peptide bond between the gamma carboxyl group of glutamate and the amino group of cysteine. That unusual bond is mechanistically important: it makes glutathione resistant to hydrolysis by typical intracellular peptidases, which is why the molecule maintains the stability needed to function as a major cellular antioxidant.
The active feature is the cysteine residue's free thiol group (-SH). That sulfur atom is what makes glutathione a powerful nucleophile and reductant — it can directly react with electrophilic compounds and oxidizing species, converting them into less reactive forms that cells can excrete. Glutathione exists in two forms: reduced (GSH, with intact thiol) and oxidized (GSSG, where two GSH molecules are joined by a disulfide bond). The ratio between these forms is one of the most important indicators of cellular redox state — typically 99% reduced GSH to 1% oxidized GSSG in healthy cells.
Calling glutathione "the master antioxidant" undersells what it actually does. Direct ROS scavenging is one role. The compound also serves as a substrate for glutathione peroxidases (which detoxify hydroperoxides), glutathione-S-transferases (Phase II detoxification enzymes that conjugate xenobiotics for excretion), and glutaredoxins (which reduce protein disulfide bonds and reverse oxidative protein modifications). It chelates heavy metals. It detoxifies acetaminophen, alcohol, and a long list of environmental toxins through liver pathways.
The roles extend beyond detoxification. Glutathione is essential for protein folding in the endoplasmic reticulum, regulates apoptosis through specific glutathionylation reactions, modulates immune cell function, and participates in cell signaling through controlled redox modifications of regulatory cysteine residues. Tissue glutathione depletion is implicated in nearly every major chronic disease category — neurodegeneration, cancer, liver disease, cardiovascular disease, kidney disease, pulmonary disease. The 2023 review in the journal of MDPI documented over 60 specific pathologies where altered glutathione homeostasis plays a mechanistic role.
Here's the honest part about glutathione supplementation: oral bioavailability is genuinely poor. The tripeptide gets broken down by gastrointestinal peptidases (slowly, due to the γ-bond, but still substantially) and the components are absorbed and resynthesized rather than the intact molecule reaching systemic circulation. This is why most published research on glutathione supplementation focuses on intravenous administration, liposomal preparations designed to bypass GI degradation, or precursor-based approaches (NAC, S-adenosylmethionine) that boost endogenous synthesis rather than supplying GSH directly.
Intravenous glutathione has a substantial clinical research history — particularly in Parkinson's disease, autism spectrum disorders, hepatic conditions, and acute drug toxicity. The mechanism is well-characterized; the clinical efficacy data is more mixed than supplement marketing suggests. For research applications studying redox biology, oxidative stress, or detoxification pathways, glutathione is foundational. For drawing conclusions about specific health outcomes from oral supplementation in humans, the literature is genuinely uneven.
Regulatory note: Glutathione has a fundamentally different regulatory status from most peptide research compounds. As an endogenous metabolite present in every cell with extensive established medical use (compounding pharmacy preparations are widely available, particularly intravenous formulations), it occupies a regulatory category outside the FDA Category 2 reclassification activity affecting BPC-157, Epitalon, and others. As both a research compound and a 503A-eligible compounding pharmacy preparation, glutathione is broadly available in the United States. WADA's Prohibited List does not specifically name glutathione as of 2025.
Here's a sourcing problem that's specific to glutathione: the cysteine thiol group that defines its bioactivity is highly vulnerable to oxidation. Exposure to atmospheric oxygen, heat, light, or trace metal contamination converts reduced GSH to oxidized GSSG progressively over time. The two forms have completely different bioactivity profiles — GSH is the active reductant; GSSG must be enzymatically reduced inside cells before it can function. Cheap suppliers routinely deliver material with significant GSSG contamination from improper synthesis, storage, or handling. The compound looks identical on basic analytical methods but contains substantially less bioactive reduced form than the label suggests. Without analytical verification specifically measuring the GSH:GSSG ratio, you may be paying for a tripeptide where most of it has already been oxidized to the inactive form.
Generic Peptides supplies research-grade Glutathione for sale at 99% purity, manufactured in the USA. Domestic synthesis with GSH:GSSG ratio verified — the part that determines whether your antioxidant assay produces published results or fails to replicate.
Order Glutathione for sale in the USA — 99% purity, verified reduced (GSH) form, manufactured domestically.
Yes — Glutathione is broadly available in the United States. Unlike most research peptides currently in regulatory transition, glutathione is widely produced by 503A compounding pharmacies (particularly for intravenous preparations) and is commercially available as both a research compound and a dietary supplement. As an endogenous tripeptide present in every cell, it occupies a different regulatory category from synthetic peptide pharmaceuticals.
Technically yes — glutathione is a tripeptide consisting of three amino acids (glutamate, cysteine, glycine). However, it has an unusual γ-peptide bond between glutamate and cysteine (instead of the standard α-peptide bond found in most biological peptides), which makes it resistant to typical peptidases. Some classification systems treat it as a peptide; others as a small molecule due to its unique chemistry.
The tripeptide is partially degraded by gastrointestinal peptidases despite the γ-bond protection. The components are absorbed and resynthesized rather than intact GSH reaching systemic circulation. This is why most research and clinical use of glutathione for therapeutic effect involves intravenous administration, liposomal formulations designed to bypass GI degradation, or precursor approaches (N-acetylcysteine, glycine, glutamic acid) that boost endogenous synthesis.
Oxidation state. GSH is reduced glutathione with an intact thiol group — this is the active antioxidant form. GSSG is oxidized glutathione, where two GSH molecules are joined by a disulfide bond between their cysteine residues. Cells continuously convert GSSG back to GSH using NADPH-dependent glutathione reductase. The GSH:GSSG ratio (typically 99:1 in healthy cells) is one of the most important measures of cellular redox state.
Probably not at the same purity or oxidation state. The cysteine thiol oxidizes easily during synthesis, storage, and handling, and cheap suppliers often deliver material with substantial GSSG contamination. Without analytical verification of the GSH:GSSG ratio, you may be paying for a tripeptide that's been substantially oxidized to the inactive form before reaching your bench. Storage matters unusually much for this compound.
Sources
Lushchak VI — "Glutathione Homeostasis and Functions: Potential Targets for Medical Interventions." Journal of Amino Acids, 2012. Comprehensive review of GSH biology, biosynthesis, and pharmacological manipulation. https://pmc.ncbi.nlm.nih.gov/articles/PMC3303626/
Aoyama K — "The Key Role of GSH in Keeping the Redox Balance in Mammalian Cells: Mechanisms and Significance of GSH in Detoxification via Formation of Conjugates." Antioxidants, 2023. Documents the molecular mechanisms of glutathione-mediated detoxification. https://pmc.ncbi.nlm.nih.gov/articles/PMC10669396/
Lubos E, Loscalzo J, Handy DE — "Glutathione: new roles in redox signaling for an old antioxidant." Frontiers in Pharmacology, 2014. Reviews GSH's role in redox signaling beyond simple antioxidant chemistry. https://pmc.ncbi.nlm.nih.gov/articles/PMC4144092/
Honda Y et al. — "Glutathione: Pharmacological aspects and implications for clinical use in non-alcoholic fatty liver disease." Frontiers in Pharmacology, 2023. Documents clinical pharmacology and intravenous administration considerations. https://pmc.ncbi.nlm.nih.gov/articles/PMC10075255/
An antioxidant tripeptide that has to stay reduced. Storage conditions are the entire molecule.
Glutathione ships as a white lyophilized powder in a sealed glass vial, freeze-dried to preserve this cysteine-containing tripeptide in its active reduced form (GSH) and extend its shelf life. Glutathione is notably more oxidation-sensitive than most peptides — cold, dark, airtight storage of the sealed vial is essential. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default — studies show freezing dramatically slows oxidation vs. refrigeration. |
| Light Sensitivity | Yes — UV and visible light accelerate the oxidation of glutathione's thiol group. | Always keep in the original box or an opaque, amber container. |
| Freezing | Allowed and strongly recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Oxidation Sensitivity | Very high. The free thiol (−SH) on glutathione's cysteine residue readily oxidizes to the disulfide form (GSSG) on exposure to air — this is the primary degradation pathway and can happen quickly once the seal is broken. | Keep the aluminum crimp cap intact until ready to reconstitute, and minimize air exposure during handling. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, darkening, clumping, visible moisture, a sticky texture, or any sulfurous odor. | Any color change, clumping, moisture, or off-smell = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
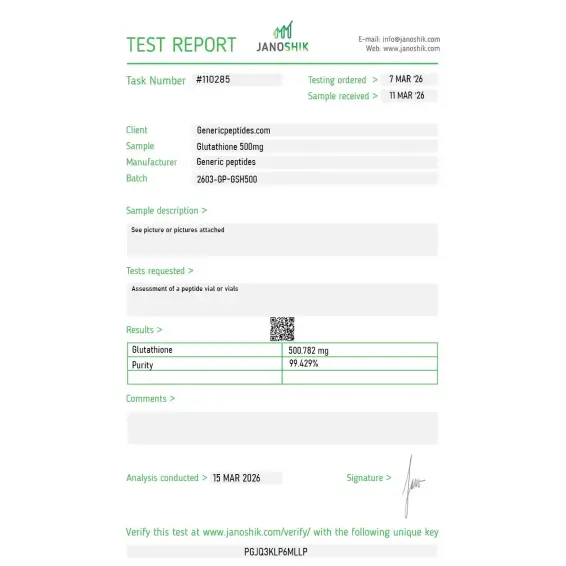
Independent lab test reports are available for Glutathione 200mg and 500mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

Works.
I switch suppliers the moment something feels off. I've been here for over a year and nothing has felt off. That's the review.
The Hopkins 1921 reference on the product page is a nice touch. Almost everything else in this catalog has either no academic context or trumped-up "discovered in 2015" claims. Glutathione has been studied longer than most modern pharmacology has existed and it's refreshing to see that acknowledged.
The product itself is fine. My only real complaint is the package — vial came wrapped in what looked like recycled bubble wrap, which is fine for shipping but contained a small tear by the time it arrived. Vial seal was intact so material was uncompromised, but the packaging could be more rigorous for a hygroscopic compound where moisture exposure during transit is a real concern. Going to keep ordering but worth mentioning.
I work primarily with the GSSG (oxidized) form for our cellular oxidation studies but ordered reduced GSH here for a comparison experiment. The catalog distinguishes the two forms clearly which sounds basic but apparently isn't — three other vendors I checked listed only "glutathione" without specifying. Small thing but it tells me the catalog is written by someone who actually knows the compound.
Honestly debated buying this directly versus making it in-house through enzymatic synthesis given the cost. Made it once, the labor cost wasn't worth it. Have been ordering here for about 11 months now, the price-to-quality tradeoff is reasonable enough that I stopped considering the in-house route.
Ordered for GST conjugation assays. Bottle arrived with desiccant intact, COA included GSH/GSSG ratio (98.4% reduced form at release), which is what I needed to see. The free thiol oxidation issue is real with this compound and not every supplier documents the ratio at release time. Three orders so far, all consistent on this metric.
Ordered for GST conjugation assays. Bottle arrived with desiccant intact, COA included GSH/GSSG ratio (98.4% reduced form at release), which is what I needed to see. The free thiol oxidation issue is real with this compound and not every supplier documents the ratio at release time. Three orders so far, all consistent on this metric.
Glutathione is a naturally occurring tripeptide — a small molecule made of just three amino acids: cysteine, glycine, and glutamic acid. It's produced in every cell of your body, with the highest concentrations in the liver, and is often called the "master antioxidant" because it neutralizes free radicals, recycles other antioxidants (like vitamins C and E), supports detoxification, and plays a critical role in immune function. Glutathione levels naturally decline with age, stress, poor diet, heavy alcohol use, illness, and exposure to environmental toxins, which is why supplementation has become increasingly popular in wellness and anti-aging medicine.
Glutathione works through several interconnected mechanisms. As an antioxidant, it directly neutralizes reactive oxygen species (free radicals) that damage cells, DNA, and proteins. In the liver, it binds to toxins, heavy metals, and drugs through a process called conjugation, making them water-soluble so they can be excreted. It also donates electrons to regenerate oxidized vitamins C and E, supports proper immune cell function, and helps regulate cell division and death. When glutathione runs low, oxidative stress rises and the body's detoxification and immune systems both weaken.
Research and clinical use suggest several benefits: reduced oxidative stress, improved liver function (especially in fatty liver disease and acetaminophen toxicity), enhanced immune function, better skin clarity and pigmentation (which has driven its popularity in Asia for skin brightening), improved insulin sensitivity, and potential benefits in Parkinson's disease, autism spectrum disorder, cystic fibrosis, and male infertility. It has also shown benefit in reducing chemotherapy-related toxicity in cancer patients. That said, the evidence quality varies significantly across conditions, and many claimed "anti-aging" and "whitening" benefits are based more on marketing than rigorous clinical trials.
Dosing varies by route and goal. For oral supplements, 250–500 mg daily is standard for general antioxidant support, with 500–1,000 mg daily used for skin-brightening or specific therapeutic goals. IV glutathione protocols typically use 600–2,400 mg per infusion, delivered over 15–30 minutes. Intramuscular injections are often given as 600 mg every other day or 1–2 times weekly. A 2017 clinical study used 300 mg oral daily for four months in fatty liver disease. Dosing should always be set by a qualified clinician, especially for IV or IM use.
There are four main routes, each with tradeoffs. IV infusion delivers the highest bioavailability (nearly 100%) and produces the fastest, most noticeable effects — but requires a clinic visit and is expensive. Intramuscular injections offer good absorption in smaller volumes and can be self-administered. Oral glutathione is convenient and inexpensive, but absorption is a real issue — standard glutathione is largely broken down in the gut before reaching the bloodstream. Liposomal and acetylated forms claim better oral absorption. Topical creams and nebulized (inhaled) forms exist for specific targets like skin and lungs.
Oral glutathione is generally well tolerated at doses up to 500 mg daily, with mild side effects including stomach cramps, bloating, and occasional allergic skin reactions. IV and IM glutathione can cause more significant reactions: a major IV skin-lightening study found liver dysfunction in 32% of patients and one case of anaphylactic shock. Other reported IV side effects include breathing difficulty, chest tightness, and abdominal pain. The Philippine FDA and similar agencies have warned specifically against high-dose IV glutathione for skin whitening due to serious safety concerns.
Yes, glutathione can lighten skin, and this has made it enormously popular across Asia — though the evidence and safety picture is complicated. Oral and IV glutathione interrupt melanin production by inhibiting the enzyme tyrosinase and shifting melanin synthesis from darker eumelanin to lighter pheomelanin. Clinical studies have shown measurable skin lightening with consistent use. However, the effect is temporary (pigmentation returns within weeks of stopping), high doses are required, and IV glutathione for whitening has been associated with serious adverse events. The FDA in multiple countries, including the US and Philippines, has specifically warned against this use.
This is one of the most debated questions. Standard oral glutathione faces a real absorption problem — it's largely broken down by enzymes in the digestive tract before reaching the bloodstream, which is why some clinicians say oral glutathione "cannot be relied upon for therapeutic purposes." However, newer formulations — liposomal glutathione (wrapped in fat-soluble spheres), S-acetyl glutathione (a stabilized form), and sublingual versions — show improved absorption in studies. Another common workaround is taking N-acetylcysteine (NAC), which your body converts into glutathione more efficiently than oral glutathione itself.
Short-term use (up to 2–3 months) at recommended oral doses has a good safety record. Long-term safety data is more limited but generally reassuring for oral use. The bigger safety concerns are with high-dose, long-term IV glutathione for skin whitening, which has been linked to thyroid dysfunction, kidney problems, severe skin reactions (Stevens-Johnson syndrome in rare cases), and liver issues. Pregnant and breastfeeding women should avoid supplemental glutathione due to insufficient safety data. Anyone with asthma should be cautious with inhaled or nebulized glutathione, which can occasionally trigger bronchospasm.
This is one of its most popular wellness uses. Your liver uses glutathione to break down alcohol's toxic metabolite acetaldehyde, and heavy drinking rapidly depletes glutathione stores. Supplementing before or after drinking may help replenish these stores and reduce oxidative damage, which is why "hangover IV drips" typically include glutathione along with B vitamins and fluids. Evidence for hangover prevention specifically is mostly anecdotal, but the underlying biochemistry is sound. For general "detox" claims, the picture is more nuanced — glutathione genuinely supports liver detoxification pathways, but your liver handles most detoxification just fine on its own in healthy individuals.
People with known asthma should avoid inhaled or nebulized glutathione due to bronchospasm risk. Those with a history of severe allergies should be cautious with IV forms, given the anaphylaxis risk documented in studies. Pregnant and breastfeeding women should avoid supplemental glutathione without specific medical guidance. Anyone with serious liver or kidney disease should consult their physician before use, since these organs metabolize and excrete glutathione. People taking chemotherapy should coordinate with their oncologist — glutathione can sometimes interfere with certain chemotherapy agents by protecting cancer cells from oxidative damage.
Researchers studying cellular redox biology and antioxidant defense often examine Glutathione alongside NAD+ (cellular energy metabolism and sirtuin activation that intersects with redox homeostasis at the mitochondrial level), 5-Amino-1MQ (NNMT inhibition that restores both NAD+ and SAM availability — the same methylation substrate that glutathione synthesis depends on), and Thymosin Alpha-1 (immune modulation research where glutathione depletion in immune cells is a documented contributor to immunosenescence).