NAD+ 100mg
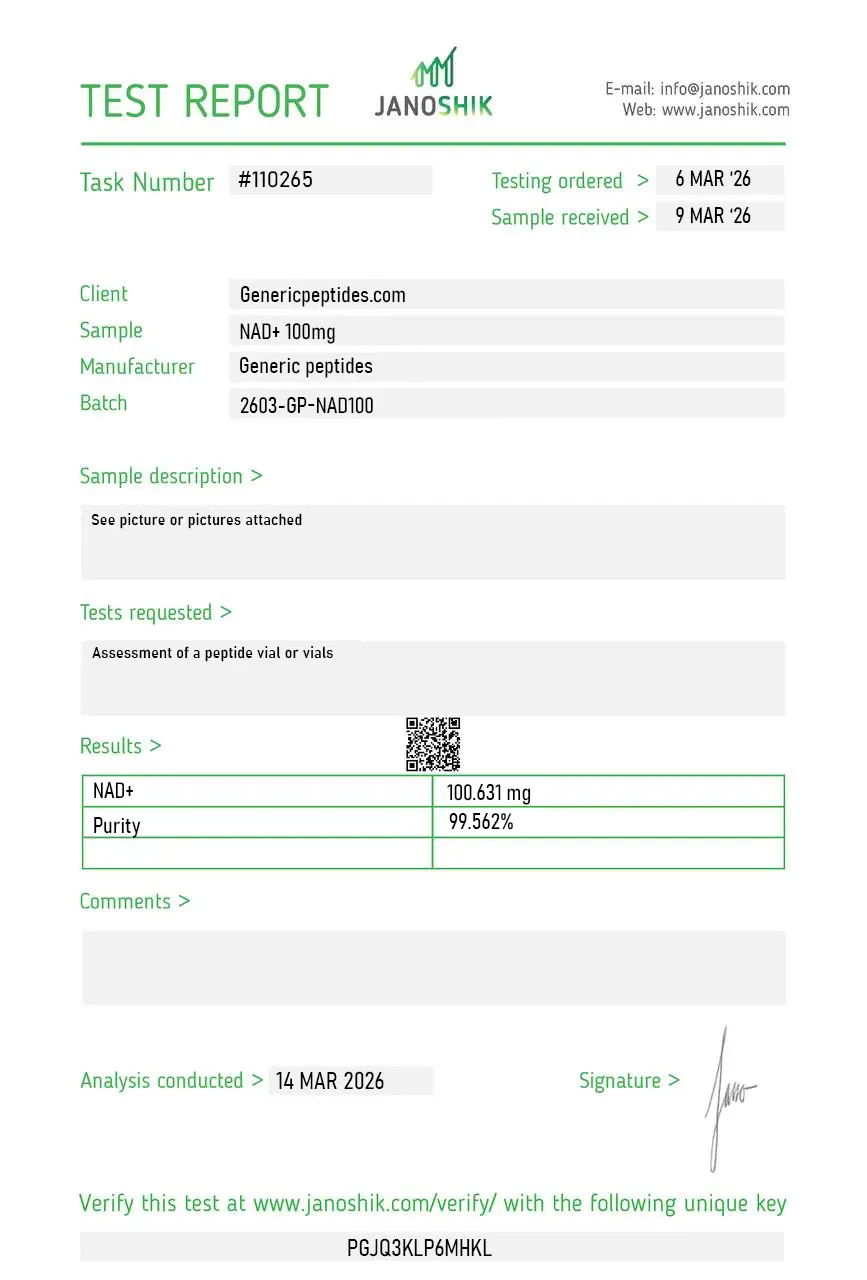
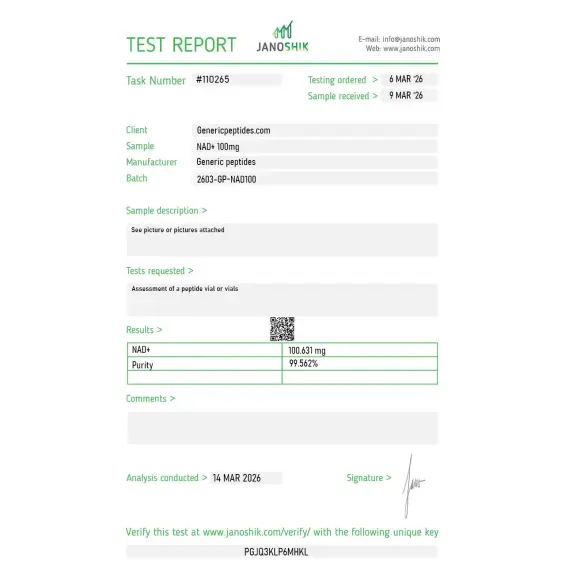
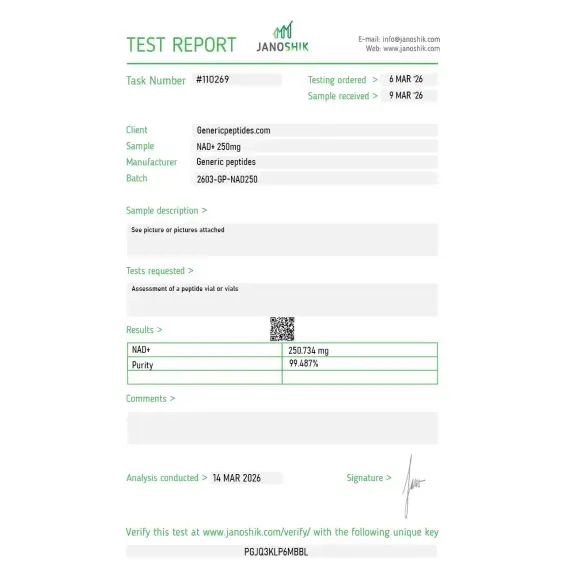
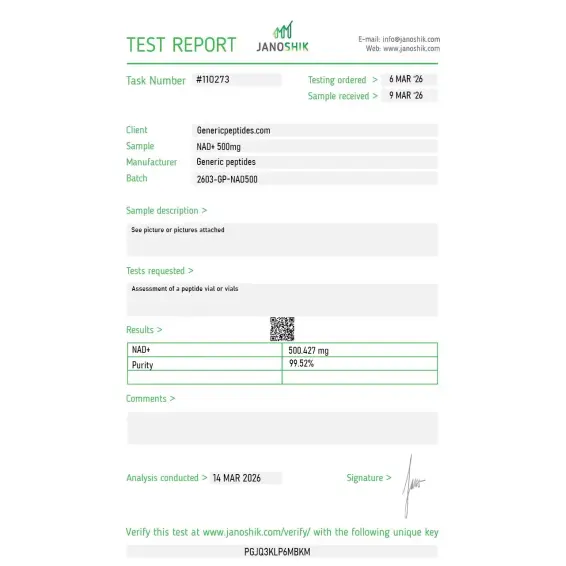
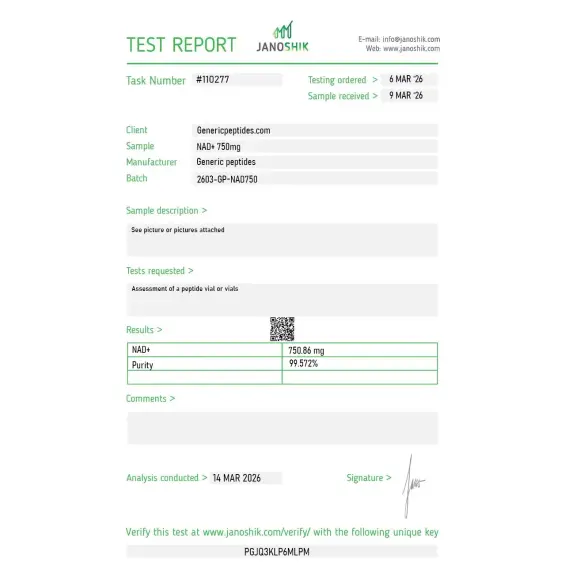
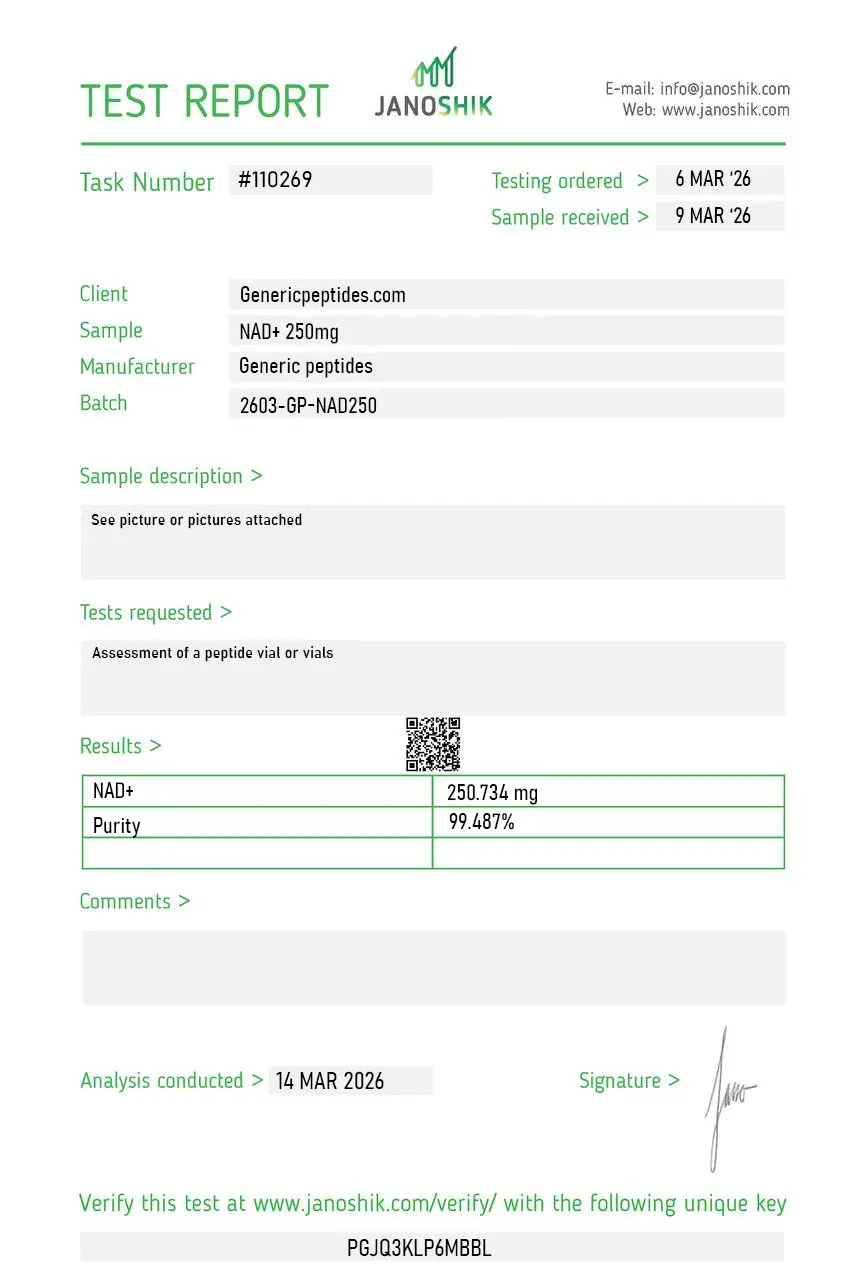
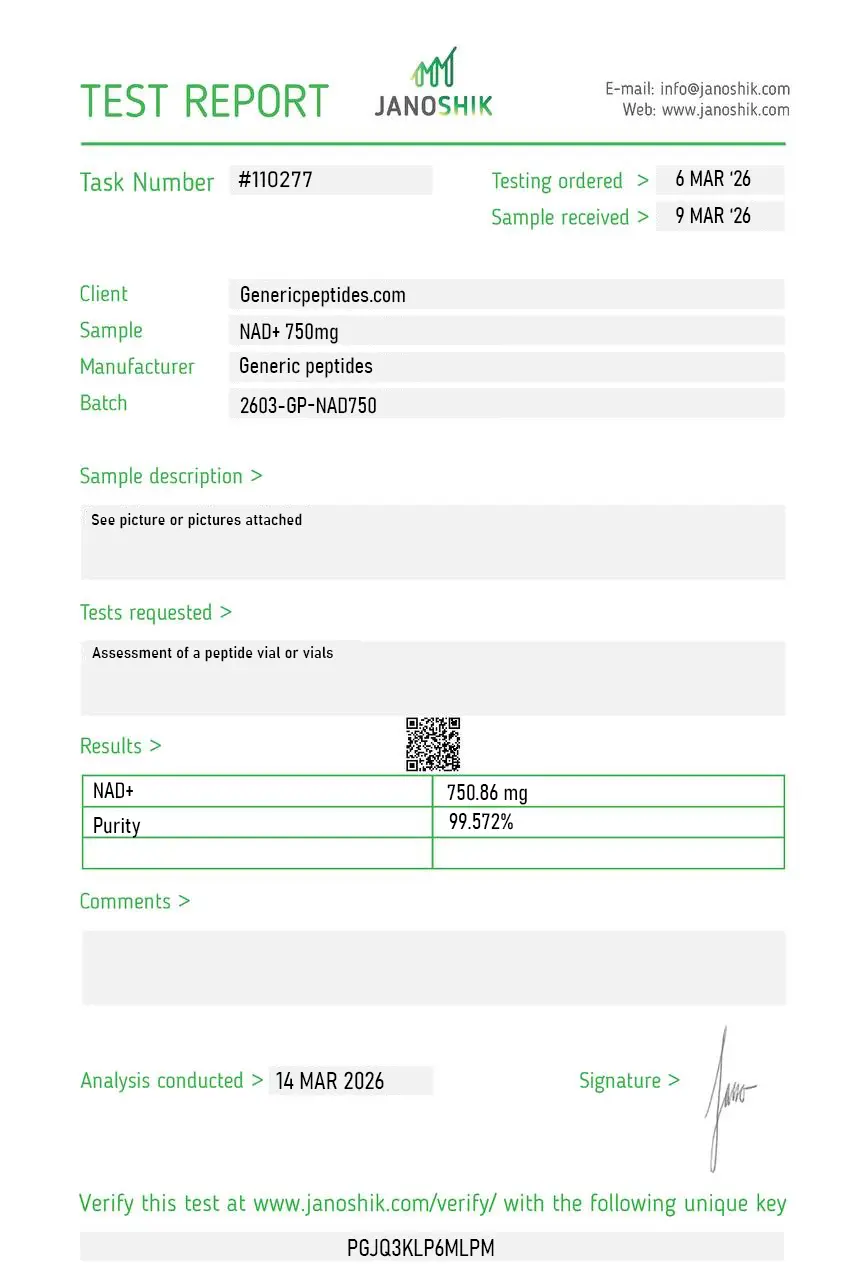
Certificate of Analysis available








Every cell in your body uses NAD+ — and the amount declines with age. By the time someone reaches 50, tissue NAD+ levels have typically dropped by 40-50% compared to their twenties — though the degree varies across tissues and individuals. This decline correlates with cellular senescence, mitochondrial dysfunction, impaired DNA repair, sarcopenia, cognitive decline, and most of the major chronic diseases of aging. The connection isn't subtle. It's one of the most reproducibly observed biological correlations in aging research — across mice, humans, and nearly every model organism studied. The compound at the center of that biology is nicotinamide adenine dinucleotide.
NAD+ is nicotinamide adenine dinucleotide — a coenzyme, not a peptide. It's a small molecule built from two nucleotides (nicotinamide mononucleotide and AMP) joined by a phosphate bridge, found in every living cell. The molecule exists in two forms: NAD+ (oxidized) and NADH (reduced). The interconversion between these forms is how cells transfer electrons during energy metabolism — every cellular respiration step, every step of the electron transport chain, every fatty acid oxidation reaction passes through NAD+/NADH cycling.
That's the textbook role. The role that turned NAD+ into the most-discussed aging compound of the past decade is different: NAD+ also serves as a substrate consumed by enzymes that govern aging biology directly. Sirtuins (the longevity-associated deacetylases). PARPs (the DNA damage repair enzymes). CD38 (the immune signaling protein that becomes hyperactive with age). All of them require NAD+ as a substrate that gets used up rather than recycled. As cellular NAD+ depletes, these enzymes lose function — and the cellular processes they govern fail with them.
The connection between NAD+ depletion and aging biology was established through decades of work. Sirtuin research from David Sinclair's lab at Harvard and Leonard Guarente's at MIT demonstrated that sirtuins regulate gene expression patterns associated with longevity — but they require NAD+ to function. As NAD+ drops with age, sirtuins go quiet. PARPs become hyperactive in response to accumulating DNA damage, consuming NAD+ in the process and depleting available pools further. CD38 expression increases with age in many tissues, accelerating NAD+ degradation in a feedback loop.
The therapeutic implication seemed clear: restore NAD+ levels and you may restore the cellular processes that depend on it. Multiple research groups developed strategies. Direct supplementation with NAD+ itself (challenging due to limited cellular uptake). NAD+ precursors like NMN (nicotinamide mononucleotide) and NR (nicotinamide riboside). Inhibitors of NAD+-consuming enzymes like 5-Amino-1MQ (NNMT inhibitor) and apigenin (CD38 inhibitor). Each approach has its own research base. NAD+ supplementation directly remains a focus particularly in research targeting acute NAD+ depletion (chemotherapy, ischemia, sepsis) where intravenous administration produces measurable tissue level increases.
Here's the honest part: NAD+ research is still working through fundamental questions. Whether direct NAD+ administration produces meaningful intracellular increases (vs being broken down extracellularly to nicotinamide and reabsorbed via the salvage pathway) remains debated. The bioavailability of NAD+ itself is poor — the molecule doesn't readily cross cell membranes, which is why precursors like NMN and NR are often preferred for systemic supplementation. The most-studied human NAD+ administration uses intravenous infusion at high doses, which is fundamentally different from oral or subcutaneous administration.
The clinical evidence is more nuanced than the supplement marketing suggests. Animal data is strong and reproducible across multiple models. Human clinical trial data on outcomes (vs surrogate markers like NAD+ levels themselves) is genuinely limited. Anyone selling NAD+ as a guaranteed anti-aging intervention is going far beyond what the literature supports. The mechanism is real; the clinical translation is genuinely active research territory.
Regulatory note: NAD+ has a fundamentally different regulatory status from most research peptides currently in transition. According to recent industry analysis (Frier Levitt, January 2026), NAD+ is specifically named alongside Sermorelin as an example of a compound that meets the statutory criteria for 503A compounding pharmacy production. It's not on the FDA's Category 2 list and wasn't part of the recent BPC-157, Epitalon, DSIP reclassification activity. As an endogenous metabolite present naturally in every cell, NAD+ occupies a different regulatory category from synthetic peptide pharmaceuticals. WADA's Prohibited List does not specifically name NAD+ as of 2025.
Here's a sourcing problem that's specific to NAD+: it's a highly unstable nucleotide-based coenzyme that degrades rapidly under improper storage conditions. Heat, light, moisture, and certain pH environments accelerate degradation, producing inactive metabolites that look identical to fresh NAD+ on basic analytical methods. The compound is also frequently sold in inconsistent salt forms (free acid vs sodium salt vs disodium salt) with different stability and solubility profiles, and cheap suppliers often deliver material that's been stored improperly during transit, has degraded during synthesis, or contains significant contamination from incomplete purification. Without analytical verification using methods appropriate for nucleotide chemistry (not peptide HPLC), the compound that arrives at your bench may be partially degraded already — which means your research data won't replicate published results regardless of how careful your experimental technique is.
Generic Peptides supplies research-grade NAD+ for sale at 99% purity, manufactured in the USA. Domestic production with cold-chain handling and nucleotide-appropriate analytical verification — the part that determines whether your NAD+ has the molecular integrity that decades of research require.
Order NAD+ for sale in the USA — 99% purity, full molecular integrity verified, manufactured domestically.
Yes — NAD+ is legally available in the United States. Unlike most research peptides currently in regulatory transition, NAD+ meets the statutory criteria for 503A compounding pharmacy production and is broadly available as both a research compound and a compounding-pharmacy preparation. As an endogenous coenzyme present in all living cells, NAD+ occupies a different regulatory category from synthetic peptide pharmaceuticals.
No. NAD+ is a coenzyme — specifically, a dinucleotide built from nicotinamide mononucleotide and AMP joined by a phosphate bridge. It's a small molecule (~664 daltons) much smaller than typical peptides, and its chemistry is fundamentally different from peptide chemistry. It's commonly sold alongside peptides in the research compound market because researchers studying metabolism and aging often investigate both.
Different molecules at different positions in the NAD+ biosynthesis pathway. NMN (nicotinamide mononucleotide) and NR (nicotinamide riboside) are NAD+ precursors — substrates that cells convert into NAD+ through specific enzymatic pathways. NAD+ itself is the active coenzyme used in cellular metabolism. Some researchers prefer precursor supplementation (NMN, NR) for systemic administration; others use NAD+ directly when the application requires the active molecule.
Multiple mechanisms compound. NAD+-consuming enzymes (PARPs, CD38) become more active with age in response to accumulating cellular damage. NAD+ biosynthesis pathways become less efficient. The salvage pathway that recycles nicotinamide back into NAD+ slows. The result is progressive depletion of cellular NAD+ pools, which feeds back into accelerated aging biology — sirtuin dysfunction, impaired DNA repair, mitochondrial decline.
Probably not at the same purity or stability. NAD+ is unstable to heat, light, and moisture, and cheap suppliers often deliver material that's already partially degraded during synthesis, storage, or transit. Without nucleotide-appropriate analytical verification, the difference between fresh NAD+ and degraded NAD+ is invisible until your experiment produces inconsistent results. Storage conditions matter unusually much for this compound.
Sources
Covarrubias AJ, Perrone R, Grozio A, Verdin E — "NAD+ metabolism and its roles in cellular processes during ageing." Nature Reviews Molecular Cell Biology, 2021. Comprehensive review of NAD+ biology and aging connections. https://pmc.ncbi.nlm.nih.gov/articles/PMC7963035/
Imai S, Guarente L — "NAD+ and sirtuins in aging and disease." Trends in Cell Biology, 2014. Foundational work on the NAD+/sirtuin connection in aging biology. https://pubmed.ncbi.nlm.nih.gov/24786309/
Yoshino J, Baur JA, Imai SI — "NAD+ Intermediates: The Biology and Therapeutic Potential of NMN and NR." Cell Metabolism, 2018. Documents the precursor approaches to NAD+ supplementation. https://pubmed.ncbi.nlm.nih.gov/29249689/
Frier Levitt — "Regulatory Status of Peptide Compounding in 2025." Industry analysis specifically naming NAD+ alongside Sermorelin as compounds meeting 503A compounding criteria. https://www.frierlevitt.com/articles/regulatory-status-of-peptide-compounding-in-2025/
A coenzyme used by every cell, depleted by every year. Stability isn't optional.
NAD+ (nicotinamide adenine dinucleotide) ships as a white to off-white lyophilized powder in a sealed glass vial, freeze-dried to preserve this coenzyme and extend its shelf life. NAD+ is notably hygroscopic and far less stable than most peptides once reconstituted — cold, dark, dry storage of the sealed vial is what protects it. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — the adenine and nicotinamide ring systems are prone to photodegradation under UV and bright light. | Always keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended for the unreconstituted powder. −20°C is standard for long-term storage; −80°C extends stability further if available. Never freeze a reconstituted solution — that permanently damages NAD+. | Freeze from the start if you won't use it within 3 months. |
| Signs of Degradation | Healthy powder is white to off-white and loose or cake-like. Watch for yellowing, browning, clumping, visible moisture, or a sticky texture — NAD+ is particularly hygroscopic and will clump quickly if the seal is broken. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a humid kitchen or bathroom, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm fully to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
Independent lab test reports are available for NAD+ 100mg, 250mg, 500mg, and 750mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

Been buying biochemistry cofactors for our lab for twelve years across several suppliers. This one's NAD+ is comparable to Sigma at a fraction of the cost. The savings on a high-consumption reagent like this add up fast when you're running enzyme kinetics across dozens of conditions.
A hundred years of biochemistry behind this molecule and people still act like it was invented by wellness influencers last year. Good to find a vendor that treats it as the foundational cofactor it is rather than an "anti-aging miracle." Material performs in our redox assays exactly as it should.
We use this for PARP activity assays in our DNA damage research. The compound has been reliable across four orders. My one note: solution stability is poor, as expected for NAD+, so we prepare fresh for each experiment. I'd suggest the product page include a brief stability note for anyone who hasn't worked with the dinucleotide before — would save some confused support emails.
Sourcing NAD+ (nicotinamide adenine dinucleotide) for sirtuin enzyme activity assays in our cellular aging research line. The compound serves as the required cosubstrate for SIRT1-SIRT7 deacetylase activity characterization in vitro — distinct from the precursor compounds (NMN, NR, nicotinamide) that require cellular conversion. The product page distinguishing direct NAD+ from precursor supplementation approaches was useful — most "NAD+ research" actually involves precursor compounds rather than the dinucleotide itself.
Sirtuin assays. Does the job
NAD+ serves two distinct roles. As a redox coenzyme, it transfers electrons during energy metabolism — cellular respiration, fatty acid oxidation, the electron transport chain, all involve NAD+/NADH cycling. As a substrate consumed by signaling enzymes, NAD+ provides the substrate for sirtuins (deacetylases regulating gene expression and longevity), PARPs (DNA damage repair), and CD38 (immune signaling). The dual role connects energy metabolism directly to aging-relevant cellular processes.
Oxidation state. NAD+ is the oxidized form; NADH is the reduced form (NAD+ has accepted two electrons and a proton). The two forms interconvert during cellular metabolism, with NAD+/NADH ratios serving as a measure of cellular metabolic state. NADH carries reducing power; NAD+ accepts electrons during oxidative metabolism. Both are essential, but they serve opposite chemical roles.
NAD+ itself doesn't readily cross cell membranes due to its size and charge. When ingested orally, NAD+ is largely broken down extracellularly to nicotinamide and other components, then reabsorbed and resynthesized through the salvage pathway. NMN and NR are smaller precursors that can enter cells more efficiently and feed directly into NAD+ biosynthesis. Direct NAD+ administration typically requires intravenous infusion at high doses to produce measurable tissue increases.
The molecule is highly unstable to heat, light, moisture, and certain pH environments. NAD+ degrades during synthesis, storage, and transit if cold-chain handling isn't maintained. Cheap suppliers often deliver material that's already partially degraded — broken down to nicotinamide, ADP-ribose, or other inactive metabolites. Detection requires nucleotide-appropriate analytical methods (not peptide HPLC), which most budget research compound suppliers don't run.
NAD+ was discovered in 1906 by Arthur Harden and William John Young. Otto Warburg's work in the 1930s established its role in cellular metabolism. The connection between NAD+ and aging emerged through sirtuin research in the late 1990s and 2000s, particularly work from Leonard Guarente's lab at MIT and David Sinclair's lab at Harvard. NAD+ supplementation as a research and clinical strategy expanded substantially in the 2010s and 2020s.
NAD+ is not currently named on the WADA Prohibited List as of 2025. As an endogenous coenzyme present in all cells and food sources, NAD+ doesn't fit standard performance-enhancing categories. Athletes subject to drug testing should consult their governing body's specific rules, but the compound's status as an essential metabolic cofactor places it outside conventional anti-doping concerns.
Nicotinamide adenine dinucleotide (the full chemical name), NAD (sometimes used loosely to refer to either NAD+ or NADH), beta-NAD+, Coenzyme I, Cozymase, and DPN (diphosphopyridine nucleotide, an older name). CAS number 53-84-9 for the free acid, 20111-18-6 for the disodium salt commonly sold commercially. Different naming conventions across literature and commercial sources.
Aging biology and sirtuin research lead by volume — particularly studies of cellular senescence, mitochondrial function, and longevity-associated gene expression. There's also active work in metabolic disease (obesity, type 2 diabetes, NAFLD), neurodegeneration (Alzheimer's, Parkinson's), DNA damage response and cancer biology, and acute applications in chemotherapy support, ischemia-reperfusion injury, and sepsis where NAD+ depletion contributes to pathology.
Different approaches to similar goals. NAD+ supplementation provides exogenous NAD+ or its precursors (NMN, NR) to increase cellular NAD+ pools. NNMT inhibition (with compounds like 5-Amino-1MQ) blocks the enzyme that wastes nicotinamide through methylation, indirectly preserving NAD+ precursor availability. Some researchers investigate both approaches as complementary — supplementation provides building blocks, NNMT inhibition prevents their wasteful degradation.
NAD+ is an endogenous coenzyme present in every cell with well-characterized biochemistry going back over a century. Most research peptides are synthetic compounds with shorter research histories and narrower mechanistic literatures. NAD+ research operates at the intersection of basic biochemistry, aging biology, and clinical metabolism — a different research tradition from the receptor-pharmacology approaches that dominate peptide research. The regulatory status, stability profile, and analytical requirements all reflect that fundamental difference.
Researchers studying cellular energy metabolism and aging biology often examine NAD+ alongside Glutathione (redox balance and detoxification), 5-Amino-1MQ (NNMT inhibition that directly restores NAD+ precursor availability), and Epitalon (telomere biology and longevity research where NAD+-dependent sirtuin activity and telomerase activation address complementary aspects of cellular aging).