IGF-1 LR3 100mcg
Certificate of Analysis available




Native IGF-1 has a half-life of about 10 minutes in human circulation. Insulin-like growth factor binding proteins grab it almost immediately and pull it out of action. Australian researchers in the early 1990s asked the obvious question: what if we engineered a version those binding proteins couldn't catch? They added 13 amino acids to the front, swapped one in the middle, and got IGF-1 LR3 with a 20-30 hour half-life. Same biological activity, completely different pharmacokinetics.
IGF-1 LR3 (Long Arginine 3 - Insulin-like Growth Factor 1) is a synthetic 83-amino-acid analog of native IGF-1, which is itself a 70-amino-acid protein. Two specific modifications turn IGF-1 into LR3: substitution of arginine for glutamic acid at position 3 (that's the "R3"), and addition of a 13-amino-acid extension at the N-terminus (the "Long" — sequence MFPAMPLLSLFVN). Together these changes reduce binding affinity for IGFBPs by roughly 100-fold.
The biological activity at the IGF-1 receptor stays intact. What changes is the pharmacokinetics — and that's the entire point. Native IGF-1 is sequestered by binding proteins so quickly that researchers struggled to study sustained IGF-1R signaling at all. LR3 evades the binding proteins, stays free in circulation, and remains receptor-available for sustained periods. It became the standard research tool for any work requiring continuous IGF-1R activation.
Francis and colleagues published the foundational structural work on LR3 in 1992. The compound transformed IGF-1 research by separating receptor pharmacology from binding protein interactions cleanly. Suddenly researchers could ask: what does sustained IGF-1R signaling actually do? Three decades of follow-up work mapped out the answers.
The 2001 Bodine et al. research established the IGF-1/Akt/mTOR pathway as central to skeletal muscle hypertrophy — work done largely with LR3 because native IGF-1 couldn't sustain the receptor activation needed to study chronic effects. That same pathway became foundational for understanding sarcopenia, recovery, and tissue regeneration biology. Cancer research has used LR3 to characterize IGF-1R-targeted oncology therapeutics. The compound's pharmacokinetic advantage produced a whole research literature that wouldn't exist otherwise.
Here's the uncomfortable truth IGF-1 LR3 marketing tends to skip: the same pharmacokinetic profile that makes the compound useful — sustained free IGF-1 in circulation — is also what makes it pharmacologically different from natural IGF-1 biology. Native IGF-1 evolved with its binding proteins; the dynamic regulation of free vs bound IGF-1 is part of how the system actually works. LR3 bypasses that regulation entirely. For receptor pharmacology research, that's a feature. For drawing conclusions about endogenous IGF-1 biology, it's a fundamental limitation that's easy to miss.
The IGF-1 system also has a complicated relationship with cancer biology. IGF-1R signaling is implicated in proliferation in multiple tumor types, which is why pharmaceutical companies have spent decades developing IGF-1R antagonists, not agonists. Sustained IGF-1R activation through LR3 is one reason the compound has stayed in research tools rather than progressing to therapeutic development.
Regulatory note: IGF-1 LR3 is not on the FDA's 503A bulks list. The FDA has treated it as ineligible for 503A compounding — it has no USP/NF monograph, isn't a component of any FDA-approved drug, and isn't on the bulks list. It wasn't part of the recent Category 2 reclassification activity affecting BPC-157, Epitalon, DSIP, and others. WADA prohibits IGF-1 and its analogs including LR3 for athletes in tested sports under category S2. Sales as a research compound continue legally.
Here's a sourcing problem that's specific to IGF-1 LR3: it's an 83-amino-acid protein with three internal disulfide bonds that hold its three-dimensional structure. Synthesis requires either solid-phase synthesis with careful disulfide formation or recombinant expression in cells with proper folding. Cheap production routinely produces material with scrambled disulfides, incorrect folding, or significant impurity content. The result is a peptide that may have the right molecular weight on a label but doesn't activate the IGF-1 receptor the way published research describes. With a protein this complex, sequence integrity isn't enough — folding integrity determines whether it works at all.
Generic Peptides supplies research-grade IGF-1 LR3 for sale at 99% purity, manufactured in the USA. Domestic production with correct disulfide formation and proper folding verified — the part that determines whether your IGF-1R binding assay actually replicates published data.
Order IGF-1 LR3 for sale in the USA — 99% purity, correct disulfide structure, manufactured domestically.
Yes — IGF-1 LR3 is legally available as a research compound in the United States. It's not on the FDA's 503A bulks list, and the FDA has treated compounded products containing it as ineligible for the 503A exemption. Not FDA-approved for human use. WADA prohibits it for tested athletes.
Two structural changes: arginine instead of glutamic acid at position 3, and a 13-amino-acid extension at the N-terminus. Same receptor, dramatically different pharmacokinetics. Native IGF-1 has a 10-15 minute half-life; LR3 has 20-30 hours. LR3 is also roughly three times more potent than native IGF-1 in published research due to reduced binding protein sequestration.
It doesn't, exactly — it works differently. The 100-fold reduction in IGFBP binding affinity means LR3 stays free in circulation while native IGF-1 gets sequestered. That's an advantage for sustained receptor activation in research models. It's also a fundamental departure from how the natural IGF-1 system regulates itself, which matters for interpreting any results.
Probably not at the same purity or with correct folding. The 83-amino-acid protein with three disulfide bonds is genuinely difficult to produce correctly. Cheap synthesis or recombinant production routinely delivers misfolded material that doesn't bind the receptor properly. Without analytical verification of disulfide structure, the difference is invisible until your assay produces nothing.
No, different molecules. MGF is a splice variant of the IGF-1 gene (sometimes called IGF-1Ec) produced locally in muscle in response to mechanical loading. IGF-1 LR3 is a synthetic analog of liver-produced systemic IGF-1 (IGF-1Ea variant). Both target IGF-1R but their tissue origins, regulatory contexts, and modifications differ entirely.
Sources
Bodine SC, Stitt TN, Gonzalez M et al. — "Akt/mTOR pathway is a crucial regulator of skeletal muscle hypertrophy and can prevent muscle atrophy in vivo." Nature Cell Biology, 2001. Foundational work on IGF-1R/Akt/mTOR signaling using LR3. https://pubmed.ncbi.nlm.nih.gov/11715018/
IGF-1 LR3 — Wikipedia summary of structural modifications, pharmacokinetics, and IGFBP binding properties. https://en.wikipedia.org/wiki/IGF-1_LR3
WADA — "Prohibited List" 2025. Documents IGF-1 and analog classification under category S2 for tested athletes. https://www.wada-ama.org/en/prohibited-list
83 amino acids. Three disulfide bonds. One folding pattern that has to be exact.
IGF-1 LR3 ships as a white lyophilized powder or cake in a sealed glass vial, freeze-dried to preserve this larger recombinant protein (83 amino acids with disulfide bonds) and extend its shelf life. With a few simple habits — cold, dark, dry — the sealed vial stays in perfect condition for its full shelf life. Here's exactly how to store it.
| Parameter | Details | Notes |
|---|---|---|
| Storage Temperature | Freezer at −20°C (−4°F) for long-term storage up to 24 months. Refrigeration at 2–8°C (36–46°F) is fine for short-term use up to ~3 months. | Original sealed vial in the freezer is the safest default. |
| Light Sensitivity | Yes — protect from direct light and UV exposure to prevent photodegradation. | Keep in the original box or an opaque, amber container. |
| Freezing | Allowed and recommended. −20°C is standard for long-term storage; −80°C extends stability further if available. | Freeze from the start if you won't use it within 3 months. |
| Structural Integrity | IGF-1 LR3 is a larger recombinant protein with a folded tertiary structure and disulfide bonds, more fragile than small peptides. | Handle the vial gently — avoid dropping, shaking, or jarring, even while frozen. |
| Signs of Degradation | Healthy powder is white to off-white and appears as a uniform cake or loose powder. Watch for yellowing, browning, grey tint, clumping, visible moisture, or a sticky texture. | Any color change, clumping, or moisture = discard the vial. |
| Common Mistakes | Leaving the vial at room temperature after delivery, storing in a frost-free freezer with temperature swings, or opening a cold vial and letting condensation form inside. | Put it in the freezer on arrival, and let sealed vials warm to room temperature before opening. |
Every order is processed quickly and shipped with full tracking. All products come directly from the official Generic Peptides supply chain — in original manufacturer packaging, carefully handled from warehouse to your door.
| Destination | Delivery Time | Notes |
|---|---|---|
| USA Domestic | 2–5 business days | Faster when local warehouse stock is selected at checkout |
| International | 10–15 business days | Tracking included; update frequency may vary by destination country |
| Order Processing | 24–48 business hours | Processing begins after payment confirmation |
| Tracking | Provided on all orders | Tracking number sent after dispatch; multiple warehouses may result in separate shipments |
This product is supplied through the official Generic Peptides distribution chain and shipped in original manufacturer packaging. Orders are packed securely to protect the contents during transit and to respect customer privacy as a standard practice.
Outer packaging is neutral and does not display product details on the exterior — a common approach to protect shipments from damage, tampering, and unnecessary exposure during delivery.
Every order includes full authenticity assurance: official Generic Peptides presentation, batch-linked lab documentation, and sealed original packaging — giving customers confidence in every purchase.
| Authenticity Feature | Details |
|---|---|
| Packaging | Original manufacturer packaging — sealed and unaltered |
| Lab Documentation | Batch-linked certificate of analysis available on request |
| Supply Chain | Sourced exclusively through official Generic Peptides distribution |
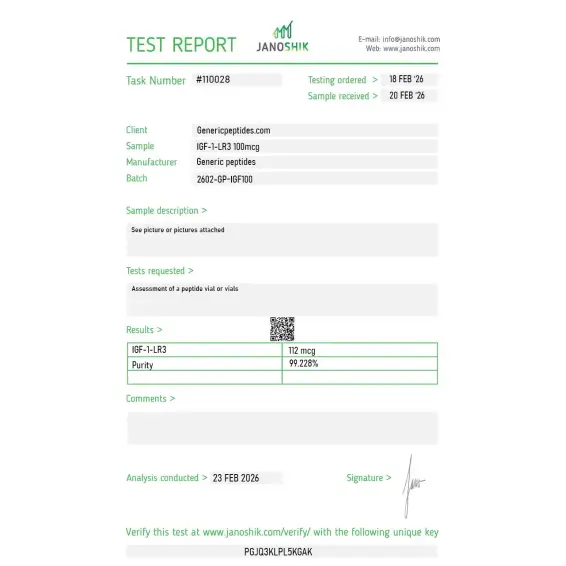
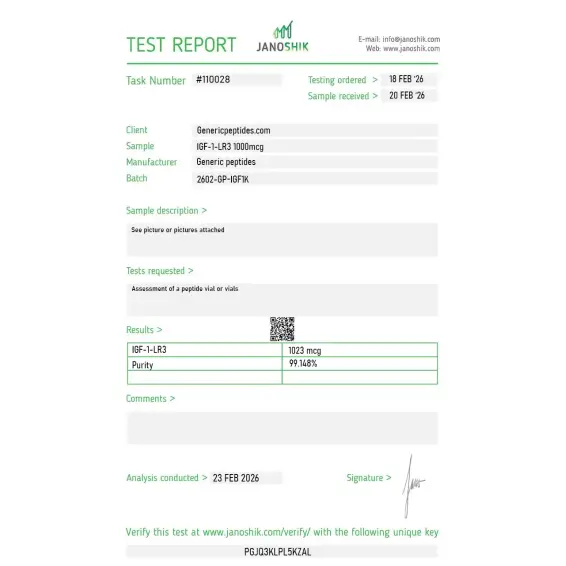
Independent lab test reports are available for IGF-1 LR3 100mcg and 1mg batches. Each certificate provides batch-level verification details, including measured content, purity result, analysis date, and report documentation.

>
Serum-free media supplementation for CHO cell bioreactor productivity. The IGFBP-resistant signaling is exactly what we optimize for in defined media — the LR3 modification is the whole point for biopharm culture. Consistent across batches.
The GroPep/Adelaide CSIRO origin is the actual heritage here — Ballard and Francis engineered LR3 specifically as a cell-culture reagent, not as a repurposed clinical compound. That's unusual and worth knowing. The listing references it. Material gave consistent proliferation responses in our assays.
For IGF-1R signaling characterization we run LR3 and watch Akt and ERK phosphorylation — the activation kinetics matched published profiles for properly folded material, no anomalous curves that would signal aggregation or misfolding. That clean signaling told me the disulfides were right. Material reliable across the conditions.
What's distinctive about LR3 is that it's a genuine industrial reagent — the biopharm industry consumes it in CHO bioreactors for monoclonal-antibody production at scale, which is a completely different market from the speculative research compounds. The listing treating it as the cell-culture reagent it actually is, rather than something else, is why I trust the sourcing. Material consistent.
Reliable in our IGF-1R reporter work. Reconstitution note for newcomers: LR3 dissolves best in dilute acetic acid, not neutral buffer — try to put it straight into PBS and you'll get incomplete dissolution and aggregation. Dilute acid first, then bring up in buffer. Material was fine following that. The listing could include the reconstitution guidance.
For comparative IGF-1-family signaling we run native IGF-1, LR3, and the DES variant side by side — different IGFBP-binding profiles, different persistence, same receptor. LR3 is the IGFBP-resistant extreme. Sourcing the family from one place keeps the comparison clean. That binding-profile contrast is the experiment.
Performs in our proliferation assays. Caution for comparative work: LR3 and native IGF-1 are not interchangeable at equal concentrations — the half-life and binding-protein resistance differ enough that you have to account for it in dosing, or your comparison is meaningless. We titrate each independently now. Material itself was fine.
The IGFBP-binding reduction is the engineering elegance — native IGF-1 is over ninety-nine percent bound by binding proteins in circulation, and the LR3 modifications free it up so it signals where native IGF-1 wouldn't. For studying IGF-1R activation without the binding-protein confound, LR3 is the right tool. Material behaved as the pharmacology predicts.
IGFBP-resistant IGF-1 analog as our standard for serum-free culture work. Consistent batches, repeated orders. Covers it.
LR3 binds the IGF-1 receptor (IGF-1R) on target cells, activating receptor tyrosine kinase activity. Downstream signaling primarily flows through two pathways: PI3K/Akt/mTOR (the major regulator of protein synthesis and cell growth) and Ras/MAPK (proliferation and gene expression). The 2001 Bodine and Rommel research established the Akt/mTOR pathway as central to skeletal muscle hypertrophy specifically.
Both are modified IGF-1 analogs but with different modifications. IGF-1 DES has the first three amino acids deleted (Des(1-3) IGF-1), which also reduces IGFBP binding. LR3 instead adds 13 N-terminal amino acids and substitutes one residue. They achieve similar pharmacological goals through different structural strategies — LR3 has the longer half-life advantage.
Three reasons combine. First, the 100-fold reduction in IGFBP binding leaves more peptide free in circulation. Second, the structural modifications shift the molecule's three-dimensional conformation enough to reduce recognition by insulin-degrading enzyme (IDE). Third, the arginine substitution alters local charge in ways that decrease matrix metalloproteinase affinity. Together these produce the 20-30 hour half-life.
The compound is a complex 83-amino-acid protein with three internal disulfide bonds essential for correct folding. Producing it correctly requires either careful solid-phase synthesis with proper disulfide formation steps or recombinant expression in cells capable of correct folding. Cheap production routinely delivers material with scrambled disulfides or incorrect three-dimensional structure that doesn't bind IGF-1R properly.
IGF-1 LR3 was developed in the late 1980s and early 1990s by researchers at GroPep (now Novozymes), an Australian biotechnology company specializing in growth factor research. The foundational structural and pharmacological characterization by Francis and colleagues was published in 1992. The compound has been continuously used in academic research for over three decades.
Yes. WADA prohibits IGF-1 and its analogs including LR3 under category S2 (Peptide Hormones, Growth Factors, Related Substances and Mimetics). The classification covers IGF-1 in all forms — native, recombinant, and engineered analogs. Athletes subject to drug testing should avoid the compound regardless of how it's obtained.
Long R3 IGF-1, LR3-IGF-1, Long Arginine 3 IGF-1, and rIGF-LR3 (when produced recombinantly). The compound is sometimes labeled simply as "IGF-1 LR3" without the hyphen. CAS number 946870-92-4. The 83-amino-acid sequence with the N-terminal MFPAMPLLSLFVN extension and Arg3 substitution identifies it unambiguously.
Skeletal muscle biology and the IGF-1/Akt/mTOR signaling pathway lead by volume — work that produced foundational understanding of muscle hypertrophy regulation. Cancer research uses LR3 to characterize IGF-1R signaling in tumor models, particularly for developing IGF-1R-targeted therapeutics. There's also active work in neuroscience (IGF-1's role in CNS development and neuroprotection) and metabolism research.
Native IGF-1 is the primary downstream mediator of growth hormone's anabolic effects — most of GH's tissue-level actions actually happen through IGF-1, which the liver produces in response to GH stimulation. LR3 directly activates IGF-1R without requiring GH stimulation, allowing researchers to separate IGF-1R-mediated effects from the broader GH signaling cascade. This separation is one of LR3's main research advantages.
Different molecules with different research applications. MGF is a splice variant of IGF-1 produced locally in skeletal muscle in response to mechanical loading and damage — believed to play a specific role in satellite cell activation. IGF-1 LR3 is a synthetic analog of systemic (liver-produced) IGF-1 with engineered pharmacokinetic improvements. Both signal through IGF-1R but their tissue origins, regulatory contexts, and structures are entirely distinct.
Researchers investigating anabolic signaling, muscle hypertrophy, and tissue repair consistently examine IGF-1 LR3 alongside compounds that target overlapping or complementary growth and recovery pathways. PEG-MGF is the most natural pairing — both derive from the same IGF-1 gene through alternative splicing, but target different receptor systems; IGF-1 LR3 signals through IGF-1R for systemic anabolic effects while PEG-MGF's E-domain activates satellite cells through a distinct receptor, making them complementary tools for dissecting local vs systemic muscle growth signaling. BPC-157 addresses tissue repair through angiogenesis and growth factor signaling at injury sites — a different molecular mechanism than IGF-1R activation but targeting similar recovery outcomes, and the two are frequently examined together in musculoskeletal repair research. TB-500 works through G-actin sequestration affecting cell motility and migration — particularly relevant for satellite cell activation research where IGF-1 LR3's proliferative effects and TB-500's migratory effects address complementary aspects of muscle regeneration. Ipamorelin and Mod GRF (1-29) stimulate endogenous GH release which drives hepatic IGF-1 production — researchers studying the GH/IGF-1 axis often examine secretagogues alongside direct IGF-1 analogs to compare indirect stimulation vs direct receptor activation.